LOS ANGELES UNIFIED SCHOOL DISTRICT
|
|
|
- Alicia Díaz Sánchez
- hace 5 años
- Vistas:
Transcripción
1 LOS ANGELES UNIFIED SCHOOL DISTRICT Owner Controlled Insurance Program The School Repair and Construction Program Insurance Manual Insurance Manual August 16, 2006 OCIP II
2 OWNER CONTROLLED INSURANCE PROGRAM Insurance Manual & Safety Standards 333 S. Beaudry Avenue Los Angeles, CA Phone (213) Fax (213) Insurance Manual August 16, 2006 OCIP II
3 Table of Contents SAFETY PROGRAM CONTRIBUTION... 2 DEFINITIONS... 2 OCIP ADMINISTRATION... 4 EXCLUDED PARTIES... 6 EVIDENCE OF COVERAGE... 6 SUMMARY DESCRIPTION OF OCIP COVERAGES... 6 CONTRACTOR BIDS ADJUSTMENTS FOR OCIP INSURANCE COSTS ENROLLMENT MAINTAINING ENROLLMENT IN THE OCIP SAFETY STANDARDS PAYROLL REPORTS INSURANCE COMPANY PAYROLL AUDIT CHANGE ORDER PROCEDURES DEMOLITION WORK CLOSE OUT AND AUDIT PROCEDURES WORKERS COMPENSATION CLAIMS LIABILITY CLAIMS AUTOMOBILE CLAIMS POLLUTION CLAIMS BUILDERS RISK CLAIMS FORMS & EXHIBITS:. 22 Insurance Manual August 16, OCIP II
4 OCIP PROJECT DIRECTORY Section 1 Overview Welcome to the LAUSD School Repair and Construction Program Owner Controlled Insurance Program. The LAUSD has arranged for its construction projects to be insured under its Owner Controlled Insurance Program (OCIP). An OCIP is a single insurance program that insures the District, the Board, all Enrolled Contractors (and their Enrolled Subcontractors), and other designated parties for Work performed at the Project Site(s). Certain Contractors and Subcontractors are excluded from this OCIP. These parties are identified in Section 3 of this Manual. Coverage under the OCIP includes Workers Compensation, Employer s Liability, General Liability, Excess Liability, Builders Risk, and Contractor's Pollution Liability Insurance for operations of Enrolled Parties at the Project Site ( OCIP Coverages ). The District will pay the insurance premiums for the OCIP coverages described in this Manual. You should notify your insurance broker/insurer(s) of the coverages provided under this OCIP for on-site activities to avoid the duplication of coverage. Each bidder is required to exclude from its bid price the cost of the OCIP Coverages provided by the District. The Contractor's and Subcontractor's cost of insurance would include the reduction in insurance premiums, related taxes and assessments, markup on the insurance premiums and losses retained through the use of a self-funded program, self-insured retention or deductible program. The total cost of insurance must include expected losses within any retained risk. The Contractor must deduct the cost of insurance for all their Subcontractors from the bid in addition to their own cost of insurance. DISCLAIMER: The information in this Manual is intended to outline the OCIP. If any conflict exists between this Manual and the OCIP insurance policies the insurance policies will govern. Insurance Manual August 16, OCIP II 1
5 OCIP PROJECT DIRECTORY Safety Program Contribution Safety on the Project Site(s) is important to the District. To encourage the participation of all Contractors and Subcontractors in Project safety, the District will require all Contractors to contribute $ to the OCIP Safety Program whenever there is a commercial general liability loss that is due to the Contractor s Work, or the acts or omissions of the Contractor or its Subcontractors, or others for whom the Contractor is responsible. The Safety Program Contribution is not covered by the OCIP Insurance Policies and is to remain uninsured by the Contractor and its Subcontractors. Definitions ELIGIBLE PARTIES Parties performing labor or services at the Project site are eligible to enroll in the OCIP unless an Excluded Party. ENROLLED PARTIES, CONTRACTORS/ SUBCONTRACTORS EXCLUDED PARTIES: Those eligible Contractors and Subcontractors that have submitted all necessary enrollment information and have been accepted into the OCIP as evidenced by a Confirmation Letter and Certificate of Insurance. Excluded Parties : (a) Hazardous materials remediation, removal and/or transport companies and their consultants; (b) Architects, surveyors, engineers, and soil testing engineers, and their consultants; (c) Vendors, suppliers, fabricators, material dealers, truckers, haulers, drivers and others who merely transport, pickup, deliver, or carry materials, personnel, parts or equipment or any other items or persons to or from the Project site; (d) Contractors and each of their respective Subcontractors who do not perform any actual labor on the Project site, during the term of the Contract; (e) Any parties or entities not specifically designated by in its sole discretion, even if otherwise eligible. Insurance Manual August 16, OCIP II 2
6 OCIP PROJECT DIRECTORY OCIP PROGRAM ADMINISTRATOR : LAUSD s Owner Controlled Insurance Program - A coordinated insurance program providing certain coverages, as defined herein, for the District, Eligible and Enrolled Contractors, and eligible and Enrolled Subcontractors performing Work at the Project Site. Aon Risk Services, Inc. Insurance Manual August 16, OCIP II 3
7 OCIP PROJECT DIRECTORY Section 2 OCIP Project Directory The following list includes key insurance personnel involved in the OCIP. OCIP Administration OVERALL PROGRAM ADMINISTRATION: Aon Risk Services, Inc. 707 Wilshire Boulevard, Suite 6000 Los Angeles, CA (213) (telephone) (213) (fax) Jim Holobaugh - Program Manager Fred Mesa Program Administrator (Primary Contact for Enrollment, Payroll, etc.) (213) (telephone) (847) (fax) Jim_Holobaugh@ars.aon.com (866) (telephone) ((800) (fax) Fred_Mesa@ars.aon.com BUILDERS RISK PROGRAM ADMINISTRATION Driver Alliant Insurance Services 1301 Dove Street, Suite 200 Newport Beach, CA Claims Office: 600 Montgomery Street, 9 th Floor San Francisco, CA Julia Gossard-Gordon Account Manager Robert Frey Claims Manager (949) (telephone) (949) (fax) jgossard@driveralliant.com (415) (telephone) (415) (fax) rfrey@driveralliant.com Insurance Manual August 16, OCIP II 4
8 OCIP PROJECT DIRECTORY LAUSD Division of Risk Management & Insurance Services 333 South Beaudry Avenue Room Los Angeles, CA (213) (telephone) Steven La Shier - Deputy Risk Manager Robert Reider - OCIP Manager Vaughan Hargrave Construction Safety Manager (Existing Construction Division) (213) (telephone) (213) (fax) Steven.Lashier@lausd.net (213) (telephone) (213) (fax) Robert.Reider@lausd.net (213) (telephone) Vaughan.Hargrave@lausd.net Chris Bartku Construction Safety Manager (New Construction Division) (213) (telephone) (213) (fax) Chis.bartku@lausd.net Insurance Manual August 16, OCIP II 5
9 OCIP INSURANCE COVERAGE Section 3 OCIP Coverages This chapter provides a brief description of OCIP Coverages. You must refer to the actual policies for details concerning coverage, exclusions and limitations. Excluded Parties Excluded Parties must meet the insurance requirements established in Section 4 and provide evidence of coverage to the District. Evidence of Coverage Each Enrolled Party will be issued a workers compensation policy. The OCIP Administrator will provide a Certificate of Insurance evidencing workers compensation, general liability, excess liability, builders risk, and contractor s pollution liability insurance to each Enrolled Contractor and Enrolled Subcontractor, each of whom will be a named insured on the OCIP policies. Complete copies of the insurance policies are available for your review in the OCIP Administrator's office Summary Description of OCIP Coverages The following descriptions on these pages provide a summary of OCIP insurance coverages ONLY. Contractors and Subcontractors should refer to the policies for actual terms, conditions, exclusions and limitations. Insurance Manual August 16, OCIP II 6
10 OCIP INSURANCE COVERAGE Each Enrolled Party will be issued a separate workers compensation policy Workers Compensation and Employers Liability: State California LIMITS OF LIABILITY Part One - Workers Compensation: Statutory Limit Part Two - Employer s Liability: Annual Limits Per Enrolled Party Bodily Injury by Accident, each accident $2,000,000 Bodily Injury by Disease, each employee $2,000,000 Bodily Injury by Disease, policy limit $2,000,000 A single policy will be issued covering all Enrolled Parties. Commercial General Liability Coverage Form-Occurrence Limits of Liability Shared by All Enrolled Parties General Aggregate $4,000,000 Products/Completed Operations Aggregate $4,000,000 Bodily Injury & Property Damage Each Occurrence $2,000,000 Personal/Advertising Injury Each Occurrence $2,000,000 Fire Damage Legal Liability $1,000,000 Medical Expense $5,000 This insurance will NOT provide coverage for products liability to any insured party, vendor, supplier, off-site fabricator, material dealer or other party for any product manufactured, assembled or otherwise worked upon away from the Project Site. Ten (10) Years Products & Completed Operations Extension beyond final acceptance of the entire project with a single, non-reinstated aggregate limit. The policy contains exclusions. Some of these exclusions are: Real & Personal Property in the care, custody or control of the insured; Asbestos; Lead; Discrimination & Wrongful Termination; ERISA; Architects & Engineers Errors & Omissions; Owned & Non-Owned Aircraft, Watercraft, Pollution and Automobile Liability; Nuclear Broad Form Liability, Terrorism Excess Liability Limits of Liability Shared by All Enrolled Parties Each Occurrence Limit $100,000,000 Annual General Aggregate Limit $100,000,000 Policy follows form (provisions, coverage, exclusions, etc.) of underlying Commercial General Liability and Employer s Liability policy wording. Builders Risk Limits of Liability Projects Under $50 Million Each Occurrence Limit $50,000,000 Deductible - Each Loss $10,000 Insurance Manual August 16, OCIP II 7
11 OCIP INSURANCE COVERAGE All projects in excess of $50 million in construction value must be submitted for individual underwriting prior to binding coverage. Contractor s Pollution Liability Limits of Liability Shared by All Insureds Each Occurrence Limit $30,000,000 Annual General Aggregate Limit $30,000,000 Contractor or Subcontractor Deductible - Each Loss $250,000 Aggregate Deductible $1,000,000 NOTE: Insurance coverage and limits provided under the OCIP are limited in scope and are specific to Work performed after the inception date of your enrollment into this OCIP. Your insurance representative should review this information. Any additional coverage you may wish to purchase will be at your option and expense. NOTE: Contractors and Subcontractors are advised to arrange their own insurance for Contractor or Subcontractor owned or leased equipment and materials. The OCIP will not cover Contractor or Subcontractor property. Insurance Manual August 16, OCIP II 8
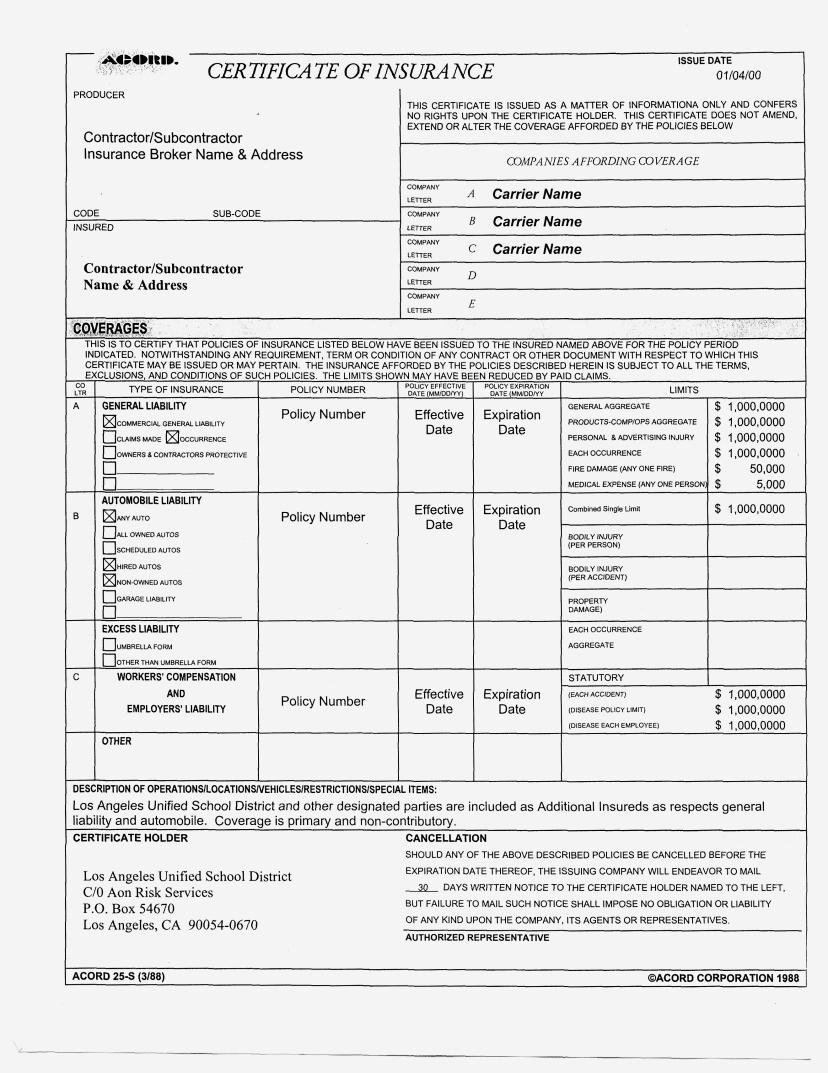
12 REQUIRED COVERAGES Section 4 Contractor and Subcontractor Required Coverage Contractors and all Subcontractors are required to maintain coverage to protect against losses that occur away from the Project Site or that are otherwise not covered under the OCIP. Contractors and Subcontractors are required to maintain insurance coverage for the duration of the Contract that protects the District from liabilities. These liabilities may arise from the Contractor s and Subcontractor s operations performed away from the Project site, from coverages not provided by the OCIP, or from operations performed by Excluded Parties. The OCIP places Contractors and Subcontractors into one of two main categories: Enrolled Parties or Excluded Parties. See Section 7 for sample Certificate of Insurance. Enrolled Parties are to provide evidence of Workers Compensation, General Liability, and Excess/Umbrella Liability insurance for off-site activities and Automobile Liability insurance for both on-site and off-site activities as per the insurance specifications in the Contract. See Section 2 for the definition of Enrolled Parties. Prime Contractors provide their Certificate of Insurance to Aon upon enrollment in the OCIP. Subcontractors provide their Certificates of Insurance to their Prime Contractor. Excluded Parties must provide evidence of Workers Compensation, General Liability, Excess/Umbrella Liability and Automobile Liability insurance for all activities including both on-site and off-site activities as per the insurance specifications in the Contract. See Section 2 for the definition of Excluded Parties. Prime Contractors provide their Certificate of Insurance to Aon upon enrollment in the OCIP. Subcontractors provide their Certificates of Insurance to their Prime Contractor. All Prime Contractors must submit verification of insurance in the form of a Certificate of Insurance on a standard ACORD form 25-S. They must provide Insurance Manual August 16, OCIP II 9
13 REQUIRED COVERAGES verification of insurance to the OCIP Administrator within ten (10) working days of Notice of Intent to Award of contract, prior to mobilization and within ten (10) days of any renewal, change or replacement of coverage. A sample of an acceptable Certificate of Insurance is provided in Section 7. Certificate of Insurance Within 5 days of Notice of Intent to Award, prior to mobilization and within ten (10) days of renewal, change or replacement of coverage, Prime Contractors will submit a Certificate of Insurance to Aon evidencing the coverage and limits as specified in this section. A 30-day notice of cancellation provision and additional insured status is required on all Certificates. Eligible Contractors shall provide evidence of workers compensation insurance for off-site activities. Excluded Parties shall provide evidence of workers compensation applicable to on and off-site projects. Eligible Contractors shall provide evidence of general liability insurance for off-site activities. Excluded Parties shall provide evidence of general liability insurance applicable to on and off-site projects and must add the District and other parties as additional insureds to their policy. Please note the requirements for thirty (30) days notice of cancellation, modification or material change. The additional insured endorsement shall state that the coverage provided to the additional insureds is primary and non-contributing with respect to any other insurance available to the additional insureds. All Contractors and Subcontractors are responsible for monitoring their Enrolled Subcontractors and Excluded Parties Certificates of Insurance. The District reserves the right to disapprove the use of Subcontractors unable to meet the insurance requirements. Certificates of Insurance evidencing compliance are to be available to the District or the OCIP Administrator upon request. The limits of liability shown for the insurance required of the Contractors and Subcontractors are minimum limits only and are not intended to restrict the liability imposed on the Contractors and Subcontractors for Work performed under their Contract. Workers Compensation and Employer s Liability Part One - Workers Compensation: Statutory Limit Part Two - Employer s Liability: Annual Limits: Bodily Injury by Accident, each accident $1,000,000 Bodily Injury by Disease, each employee $1,000,000 Bodily Injury by Disease, policy limit $1,000,000 Commercial General Liability/Umbrella Liability Limits of Liability General Aggregate $1,000,000 Products/Completed Operations Aggregate $1,000,000 Personal/Advertising Injury Aggregate $1,000,000 Each Occurrence Limit $1,000,000 Coverage must be an Occurrence form and it must apply to bodily injury and property damage for operations (including explosion, collapse and underground coverage), independent contractors, products and completed operations. Limits can be provided by a combination of a primary Commercial General Liability policy and an Excess or Umbrella Liability policy. Insurance Manual August 16, OCIP II 10
14 REQUIRED COVERAGES All Contractors and Subcontractors shall provide evidence of automobile liability. The OCIP does not cover automobile liability. Automobile Liability A Commercial Business Auto Policy which covers all owned, hired and nonowned automobiles, trucks and trailers with coverage limits not less than $1,000,000 Combined Single Limit each accident for bodily injury and property damage. Coverage will apply both on and away from the Project Site(s). All Subcontractors shall be required to maintain limits of not less than $1,000,000 Combined Single Limit. Property Insurance Contractors and Subcontractors are advised to arrange their own insurance for owned and leased equipment, whether such equipment is located at a Project Site or in transit. Contractors and Subcontractors are solely responsible for any loss or damage to their personal property including contractor tools and equipment, scaffolding and temporary structures, whether owned, used, leased or rented by the contractor. Contractors and Subcontractors are also responsible for any loss or damage to property or materials created or provided under the Contract. Watercraft and Aircraft Liability The operator of any watercraft or aircraft of any kind must maintain liability naming the District and the respective Contractor and/or Subcontractor as an additional insured with primary and non-contributory wording. In addition, the limit of liability must be satisfactory to the District. Such insurance requirements will be determined as the need arises. The District does not provide professional liability insurance. Professional Liability All professional service firms must provide professional liability insurance appropriate for their profession and satisfactory to the District. Pollution Liability Asbestos Contractors and Subcontractors whose Work involves removal or treatment of asbestos must provide and maintain an asbestos abatement endorsement to their general liability and excess liability policies. Such coverage will specifically schedule the type of work defined in the Contract. The District will determine limits based on the nature of the contract and the risk involved. Insurance Manual August 16, OCIP II 11
15 REQUIRED COVERAGES Note: Waivers Required The Contractor's Workers Compensation, General Liability, Automobile Liability and Umbrella or Excess Liability insurers shall provide Waivers of Subrogation in favor of the District and other designated parties. General Liability and Excess Liability Insurance policies will name the District, the Board, its officials, employees and agents and the OCIP Administrator as additional insureds and it will state that the coverage is primary and noncontributory. Insurance Manual August 16, OCIP II 12
16 CONTRACTOR-RESPONSIBILITIES Section 5 Contractor and Subcontractor Responsibilities Throughout the course of the Project(s), Contractors and Subcontractors will be responsible for reporting and maintaining certain records as outlined in this section. The Contractors and Subcontractors are required to cooperate with the District and its OCIP Administrator in all aspects of OCIP implementation and administration. Responsibilities of the Contractor include all contract responsibilities, and the following: Safety Pre-Qualification prior to submitting a bid. Contractors may only contract with Subcontractors that they have safety pre-qualified Excluding the cost of OCIP insurance from their bids, if eligible for the OCIP Providing each Subcontractor with a copy of this Insurance Manual & Safety Standards Enrollment in the OCIP, if eligible, within ten (10) working days of notice of intent to award of contract Including OCIP provisions in all contracts with Subcontractors Providing timely evidence of other insurance or contractor required insurance to the OCIP Administrator within ten (10) working days of notice of intent to award of contract Notifying the OCIP Administrator of all subcontracts awarded Maintaining and reporting monthly payroll records Cooperating with the OCIP Administrator s requests for information Complying with insurance, claim and safety procedures Monitoring its Subcontractor's Certificates of Insurance Notifying the OCIP Administrator immediately of any insurance cancellation, modification, material change or non renewal of Contractor required insurance Insurance Manual August 16, OCIP II 13
17 CONTRACTOR-RESPONSIBILITIES Responsibilities of Subcontractors of all tiers: Enrollment in the OCIP, if eligible Safety pre-qualification Maintaining and reporting monthly payroll records Cooperating with the OCIP Administrator's requests for information Complying with insurance, claim and safety procedures Monitoring its Subcontractor's Certificates of Insurance See Section 7 for sample forms that can help identify your insurance costs. See Section 2 for information on contacting the OCIP Administrator. Contractor Bids The District provides insurance for all Enrolled Contractors and Enrolled Subcontractors under the OCIP for Work performed at the Project Site(s). The section below, Adjustments for OCIP Insurance Costs describes the procedure for bidding, and how you must identify the cost of insurance and then exclude your insurance costs from the bid. Section 7 of this Manual contains worksheets that can help you estimate your insurance costs for this Project. The OCIP Administrator can also assist you in identifying the insurance costs. Adjustments for OCIP Insurance Costs Each Contractor and Subcontractor is required to exclude the Costs of OCIP Coverage s from its bid price for the proposed scope of work (including subcontracted work whether or not the Subcontractor is identified at the time of the bid). Costs of OCIP Coverages is defined as the amount of Contractor s and its Subcontractors reduction in insurance costs due to eligibility for OCIP Coverages as determined by the Owner using Aon Form-1 and Aon Form-2 located in the Insurance Manual and information available to the District and/or the OCIP Administrator regarding the costs of similar coverages taking into account limits of liability, coverages, and rating of the insurer. The Contractor's and Subcontractor's cost of insurance would include the reduction in insurance premiums, related taxes and assessments, markup on the insurance premiums and losses retained through the use of a self-funded program, self-insured retention or deductible program. The total cost of insurance must include expected losses within any retained risk. The Contractor must deduct the cost of insurance for all their Subcontractors from the bid in addition to their own cost of insurance. Insurance Manual August 16, OCIP II 14
18 CONTRACTOR-RESPONSIBILITIES To aid the Contractor and its Subcontractors in identifying its workers compensation, employer s liability insurance, general liability insurance, excess liability insurance, builders risk insurance and contractor s pollution liability insurance costs the Insurance Credit Worksheet form (Aon-1), is included in Section 7 as a sample to assist the Contractor and Subcontractor in determining the cost of insurance to be deducted from the bid. A separate form can be used for the Contractor s self-performed work, each identified Subcontractor and for unidentified Subcontractors at the time of the bid. The worksheets are to assist the Contractor in removing the insurance costs from their competitive bid. Do not include these worksheets with the bid submission. Each Enrolled Contractor and Enrolled Subcontractor may be required to submit insurance documentation that supports the Cost of OCIP Coverage s deducted from the bid. Documentation may include the following pages from the Workers Compensation, Employer s Liability, General Liability, Excess Liability, Builders Risk and Contractor s Pollution Liability (as applicable) policies: Declarations or information page Rate page(s) Deductible endorsements Verification of experience modification(workers Compensation only) 5 Years of loss history for entities that retain losses Change orders must be priced by the Enrolled Parties to exclude the cost of insurance. Under the District s OCIP, the final payroll is determined by an audit by the OCIP insurer. The audited contract information will be used to calculate the Contractor s and Subcontractor s true insurance costs (in the absence of the OCIP). If the results of this comparison demonstrate that the final, actual payrolls would have produced a different deduction for insurance costs, an additional amount will be withheld from the Contractor s payments under the Contract. Contractors are solely responsible for ensuring that their Subcontractors of all tiers also deduct the cost of insurance from their bid. See Section 7 for sample OCIP forms. Enrollment Each Enrolled Contractor shall provide details about its Subcontractors to the OCIP Administrator, in order to enroll them in the OCIP. The Contractor and Subcontractor must complete and submit the Enrollment Application form (Aon-3); a sample is included in Section 7. This form must be completed and submitted to the OCIP Administrator within 10 working days of notice of intent to award contract award and prior to mobilization on the Site(s) to obtain coverage under the OCIP. Insurance Manual August 16, OCIP II 15
19 CONTRACTOR-RESPONSIBILITIES A separate Enrollment Application form (Aon-3) is required for each Eligible Subcontractor of any tier, which performs Work at the Project Site. A separate Workers Compensation policy will be issued to each Enrolled Contractor and Enrolled Subcontractor. Each Enrolled Contractor or Enrolled Subcontractor will receive a Confirmation Letter. A Confirmation Letter is a letter issued by the OCIP Administrator that confirms acceptance of the applicant into the District OCIP. Note: Enrollment is not automatic Enrollment into the OCIP is required, but not automatic. All Eligible Contractors and all Eligible Subcontractors MUST complete the enrollment forms and participate in the enrollment process for OCIP coverage to apply. Access to the Project Site will not be permitted until Enrollment into the OCIP is complete. Maintaining Enrollment in the OCIP If you do not comply with all the terms of this Manual in a timely manner, including the Construction Safety Standards, you may not remain enrolled in the OCIP. Contractors eligible for enrollment in the OCIP who are not enrolled in the OCIP will not be granted access to the Project Site(s). Safety Standards establish minimum standards for contractor safety programs. Safety Standards are provided to all participants during the bidding process. Safety Standards Each Contractor and Subcontractor is required to have a written safety program and to provide a designated safety representative who is on Site when any Work is in progress. If there are fifty (50) workers or more on a job-site, the Contractor shall have a DEDICATED, FULL-TIME, Safety Representative that has no other tasks other than administering the Contractor s and LAUSD s Safety Programs. Safety Representative requirements are as specified in the contract and LAUSD Safety Program. Minimum standards for Contractor safety programs are outlined in the LAUSD s Safety Standards. Payroll Reports Each Enrolled Contractor and Enrolled Subcontractor of every tier must submit monthly payroll reports. The reports will identify worker-hours and payroll by workers compensation classification code for all Work performed at the Project Site. This Insurance Manual August 16, OCIP II 16
20 CONTRACTOR-RESPONSIBILITIES information will be used to provide the District's insurers with information required for determining the District's premium. All Enrolled Contractors and Enrolled Subcontractors must submit payroll reports prior to the 10 th of the following month. Payroll Report form (Aon Form-4), provided in Section 7, is the only acceptable form. The monthly worker-hour and payroll reports should include supervisory and clerical personnel that are on-site and cover all Work performed at or emanating directly from each Project Site. The payroll report (Aon Form-4) for the prime contractor and all subcontractors must be submitted with the contractors request for payment. The District will not process payment requests unless the Aon Form-4 payroll report is attached. Insurance Company Payroll Audit Each Enrolled Contractor and Enrolled Subcontractor is required to maintain payroll records for each Contract. Such records will allocate the payroll by Workers Compensation classification(s) code and exclude the excess or premium paid for overtime (i.e., only the straight time rate will apply to overtime hours worked). Furthermore, such records will limit the payroll for Executive Officers and Partners/Sole Proprietors to the limitations as stated in the state manual rules. It is important that you properly classify payrolls, as these are reported to the rating bureau for promulgation of future Experience Modifiers for your firm. All Enrolled Contractors and Enrolled Subcontractors shall make available their payroll records, vouchers, contracts, documents, and records, of any and all kinds, to the auditors of the OCIP insurer(s) or the District s representatives. Availability of records must be for the policy period, any extension, or during a final audit period as required by the insurance policies. Note: Failure to submit the payroll reports as required may result in the withholding of contract progress payments or final payment until the reports are received as well as being barred from future opportunities with the District. Change Order Procedures Change orders must also exclude the Enrolled Contractor's Costs of OCIP Coverage s for the insurance coverages that are provided by the District in the OCIP. Insurance Manual August 16, OCIP II 17
21 CONTRACTOR-RESPONSIBILITIES Demolition Work As respects to demolition on any structures of 4 (four) stories or greater in height, contractors should notify the Administrator (Aon) so that notification to Liberty Mutual can be made at least 4 (four) weeks in advance of the actual work beginning. Such notification shall give Liberty Mutual Loss Prevention the option to participate in the review, pre-planning and monitoring process for the demolition work. Close Out and Audit Procedures The Enrolled Contractor and Enrolled Subcontractors must submit the Notice of Work Completion form (Aon-5), when a Contractor and/or a lower tier Subcontractor has completed its Work at the LAUSD School Repair and Construction Program Project Site (s) and no longer has workers on Site. The Aon-5 form will initiate the final payroll report and audit of payroll and worker-hours by the OCIP Insurer. The OCIP Insurer is the insurance company named on the policy or on the Certificate of Insurance that provides coverage for the OCIP. A copy of the Notice of Work Completion form, (Aon-5) with instructions on the proper method for completion is found in Section 7. Issuance of final payment will not be authorized by the District until all necessary forms have been submitted to the OCIP Administrator. Any Safety Program Contributions for which the Contractor or Subcontractor of any tier is responsible will be considered at the time of close-out. Safety Program Contributions previously paid will not be considered as a part of the close out. Insurance Manual August 16, OCIP II 18
22 CLAIM REPORTING PROCEDURES Section 6 Claim Reporting Procedures This section describes the basic procedures for reporting various types of claims: workers compensation, liability, and damage to the Project (Builders Risk). A Claims Kit will be provided to all Contractors. It will include details about claim reporting and is intended for use at the job site. Workers Compensation Claims The main responsibility for any Contractor and Subcontractor is first to see that the injured worker receives immediate medical care. Next, you should immediately notify the OCIP Administrator in the event of a serious injury or accident. To assist you in reporting an injury or accident, we have established a dedicated toll free telephone number. Please immediately report any injury using the toll free telephone number: You may report your WC First Reports of Injury 24 hours a day/365 days per year. When calling in you will need to know the school name and address. Also attached to this manual is the MPN notice. This Notice must be given to each employee to review and then must be signed for knowledge of receipt. When you report the workers compensation injury, using the special reporting telephone number, the insurance company will complete the Employer's First Report of Injury (form 5020) and make the necessary filings. It is the employer's responsibility to provide the injured worker with the Employee's Claim (form DWC-1). A copy of the employee's claim form and the Supervisor's Report of Injury form must be provided to the insurance company. The OCIP Administrator will provide Claims Kits to all Enrolled Contractors and Enrolled Subcontractors. These kits will include appropriate claim forms and postings. Additional kits or claims forms can be obtained from the OCIP Administrator or the carrier s claims coordinator. Insurance Manual August 16, OCIP II 19
23 CLAIM REPORTING PROCEDURES The District s workers compensation insurer has arranged with authorized medical providers and facilities for treatment of all minor or non-life threatening injuries. The name, address and telephone number of the nearest authorized clinic and hospital for the designated school location will be on the Posting Notice, which is in the Claims Kit. The posting notice was also sent to you at the time Aon Risk Services advised you of the completion of the enrollment. Contractors and Subcontractors must designate a representative at the site to take injured employees to the medical treatment center and to report the claim. This individual is to remain with the injured employee at the medical treatment center while he/she is being treated. The treating physician should provide a written description of whether or not the injured employee can return to work, a list of restrictions if any, and the estimated length of time the injured worker must be on modified duty. The District supports transitional modified work to keep injured workers gainfully employed during recovery. The District s workers compensation insurer will arrange with the local 911 emergency ambulance services for response to any serious traumatic life threatening injuries and will provide information in the Claims Kit. Report all Liability claims to Liberty Mutual. Liability Claims Accidents at or around the Project Site(s) resulting in damage to property of others (other than your own work product), or personal injury or death to a student, faculty member or a member of the public, must be reported immediately to Liberty Mutual by calling the toll free telephone number: Do not voluntarily admit liability. Cooperate with the District and the OCIP insurer representatives in the accident investigation. The District will assess the Contractor $500 for any damages/injuries caused by the Contractor or its Subcontractors to third parties. See the discussion on Safety Program Contribution in Section 1 of this Manual. Report all Auto claims to your insurance carrier and the OCIP Administrator. Automobile Claims No insurance coverage is provided for automobile accidents under the OCIP. It is the sole responsibility of each Contractor and Subcontractor to report accidents/claims involving their automobiles to their own insurers. However, all accidents occurring in or around the job site must be reported to the OCIP Administrator. The accident will be investigated to determine any liability arising out of the project construction activities that could result in future claims (i.e., due to the conditions of the roads, etc.). Each Contractor and Subcontractor shall cooperate in the investigation of all automobile accidents. Insurance Manual August 16, OCIP II 20
24 CLAIM REPORTING PROCEDURES Pollution Claims The District's OCIP policies may provide coverage for certain pollution conditions. Incidents must be reported promptly in writing. Report incidents or possible claims by immediately notifying the OCIP Administrator of any known or suspected pollution incidents. Builders Risk Claims All risk of direct physical loss or damage excluding earthquake and flood is subject to policy terms, conditions and exclusions. Driver Alliant is the broker for the Builders Risk program. To report claims contact: Claims Manager Robert Frey Claims Office: 600 Montgomery Street, 9 th Floor San Francisco, CA (415) (telephone) (415) (fax) RFrey@driveralliant.com Insurance Manual August 16, OCIP II 21
25 FORMS Section 7 Forms This section contains the forms needed for enrolling into the OCIP, reporting claims, reporting payroll and overall administration of the OCIP. This section contains the following forms: Aon 1 Aon 2 Aon 3 Aon 4 Aon 5 Exhibit 1 Exhibit 2 Exhibit 3 Exhibit 4 Exhibit 5 Insurance Credit Worksheet Insurance Summary Enrollment Application On-Site Payroll Report Notice of Work Completion Sample Certificate of Insurance Workers Compensation First Report of Injury or Illness General Liability Notice of Occurrence/Claim Property Loss Notice Liberty Mutual Medical Provider Network Information Note: For assistance in completing these forms, please contact the LAUSD OCIP Administrator Aon Risk Services (866) Insurance Manual August 16, OCIP II
26 Form-1 INSURANCE CREDIT WORKSHEET (Instructions located on the following page) LAUSD Page 1 of 1 1. Contractor Information: Federal ID No.: Company Name & dba / Contact Name & Title: Address: City, State Zip Code: Telephone: Fax: u Business Information (headquarters) u Contact Information (address questions to..) 2. Bid Information: Bid Package No.: Scope of Work: Proposed Contract Price: $ Amount of Self Performed Work: $ Contractor If Subcontractor, Are you a: Subcontractor identify under contract with: Workers Compensation Insurance Information: State Class Code Description Rate (per $100 payroll) Worker-hours Payroll WC Premium (Payroll * Rate / 100) 9. Totals 10. Your Company s Workers Compensation Experience Modifier: 11. Modified Premium (Total WC Premium multiplied by line 10): 12. a) Employers Liability Rate: b) Employers Liability Cost = line 11 x line 12a: 13. a) Modification Premium Factors: b) Rate c) Amount Modifier 1: Modifier 2: d)total Modified Amount: 14. Total Workers Compensation Premium (line 11 plus 12 minus 13): 15. a) General Liab. Rate: b) Based On: c) Rate factor: Payroll Per $100 GL Premium Receipts Per $1,000 Other Cost: 16. a) Builder s Risk/Installation Floater Rate: b) Property Premium Costs: Not applicable 17. a) Excess/Umbrella Rate: b) Based On: c) Rate factor: Payroll Per $100 Receipts Per $1,000 Excess/Umbrella 18. Total of all Insurance Premiums (total of lines 14, 15, 16 & 17): 19. Overhead & Profit on Insurance Prem. %: O/H & Profit Amount: 20. Total Initial Insurance Credit (Total of lines 18 &19): 21. Initial Insurance Composite Rate (line 20 divided by total payroll in line 9): Name: Title: (please print) Date: Signature:
27 INSTRUCTIONS FOR INSURANCE CREDIT WORKSHEET (AON FORM-1) A separate form may be used for each contractor, known Subcontractor and trade not currently awarded to a Subcontractor. This form may be used to estimate the cost of insurance, which must be deducted from the bid. Duplicate this form as needed: 1. Contractor Information: Provide your company's Federal ID Number. Provide your Business Information including the Company Name, Address, City, State, Zip Code, Telephone and Fax in the column. Provide the name of your employee that can answer insurance questions. If this person s Business Address, Telephone and Fax is different enter this information in the column provided. 2. Bid Information: Provide the Bid Package Number assigned by District. Provide a brief description of the work your firm will perform. Identify your proposed contract price. Identify the amount your firm will self-perform (100% if no subcontractors are used) Check the box that applies to your status on this bid. Identify with whom you are contracting (the District or the name of the contractor or subcontractor) Workers Compensation Insurance Information: Description of Worker s Compensation Column Information State & Class Code Provide the state in which the work will be performed and the workers compensation classification codes that are applicable to the scope of your work. Description Provide the workers compensation class code description that applies to the code. Rate Enter the rate your firm pays for coverage for each class code. This information can be obtained from your workers compensation policy. Worker-hours Provide your estimated worker-hours, by class code, for work that will be performed on-site. Payroll Provide your estimated payroll, by class code, for work that will be performed on-site. WC Premium For each classification you entered, multiply the Payroll by the Rate and divide by Totals Calculate totals for columns numbered, and. 10. Workers Compensation Experience Modifier - Enter your experience modification factor. This number is located on your workers compensation policy or on the Bureau s rating sheets. If you do not have an experience modifier, use Modified Premium Multiply the total on line 9 by your workers compensation experience modifier. 12. Employers Liability Rate (a) Enter your Employers Liability Rate located on your workers compensation policy and (b) calculate by multiplying the Modified Premium by the rate. 13. Modification Premium Factors Identify the premium modification factors that apply to your workers compensation policy. These factors may include a Scheduled Credit or a Premium Discount. a) Identify the name of the Modifier, (b) enter the Rate, (c) compute the Amount by calculating the Modified Premium by the Rate. Total the amount computed in column 13.c). Enter the total in 13.d). 14. Total Workers Compensation Premium Add the Modified Premium and the Employers Liability Premium (line 11 and 12). Subtract the Premium Modifications identified and totaled in line 13 d). Other Insurance Items: 15. General Liability (a) Enter the General Liability rate, (b) identify the basis the rate applies to by checking the box (if the basis is other, identify in the space provided), (c) Check whether the rate factor is ($100 or $1,000). Compute the General Liability Premium by using the formula (rate basis * rate / rate factor). 16. Builder s Risk/Installation Floater (a) Enter the rate and (b) apply to the Proposed Contract Cost identified in the Bid Information Section. 17. Excess/Umbrella Liability (a) Enter your Excess or Umbrella Liability rate, (b) identify the basis the rate applies to by checking the box (if the basis is other, identify in the space provided), (c) Check whether the rate factor is $100 or $1,000. Compute the Excess or Umbrella Liability Premium by using the formula (rate basis * rate / rate factor). Total Insurance Premiums: 18. Total of all Insurance Premiums Add lines 14, 15, 16 and Overhead & Profit (a) Identify the percentage of Overhead & Profit included in your pricing structure, (b) apply the percentage to Overhead & Profit to the Total of all Insurance Premiums. 20. Total Initial Insurance Credit Add lines 18 and Initial Insurance Composite Rate - Divide the Total Initial Insurance Credit (line 20) by the Total Payroll (column 9).
28 Form-2 INSURANCE SUMMARY LAUSD Page 1 of 1 1. Name of Contractor: 2. Bid Package No.: 3. Total Proposed Cost: $ Contracting Parties & Trades Aon Form-1 Reference No. 4. Contractor : A B C D Estimated Estimated Payroll Initial Insurance Amount of Contract Worker-hours Credit List Additional Trades NOT yet assigned to a sub (attach separate Aon Form 1 5. Your Known Subcontractors (Attach a Separate Aon Form-1 from each) 7. Total Estimates for Contract: 7a 7b 7c 7d 8. Composite Rate for Contract: (line 7d divided by line 7c * 100)
29 INSTRUCTIONS FOR INSURANCE SUMMARY (AON FORM-2) Make a separate entry on the Aon Form-2 for each contractor, known Subcontractor and trade not currently awarded to a Subcontractor. Duplicate this form as needed: General Information 1. Name of Contractor Enter the name of the Contractor or Subcontractor that is being summarized on the form. 2. Bid Package No. Enter the Bid Package No. the District assigned to the bid. 3. Proposed Contract Cost Enter the Proposed Contract Cost for the Contractor or Subcontractor being summarized. Contractor Specific Information 4. Contractor Enter the Contractor or Subcontract that is being summarized (include only self-performed work from the Aon Form-1) b) Estimated Worker-hours (line 9 and column) c) Estimated Payroll (line 9 and column) d) Initial Insurance Credit line 21). 5. Known Subcontractors For each Subcontractor summarize their work and the work of lower level tiers. Information will be obtained from either an Insurance Summary Aon Form-2, if lower level tiers were used, or the Aon Form-1. The Aon Form-1 reference numbers are supplied below: a) Amount of Contract The Proposed Contract Cost from Bid Information Section (2). b) Estimated Worker-hours The work performed by the Subcontractor and all lower level subcontractors. Information from line 9 and column 6. c) Estimated Payroll The work performed by the Subcontractor and all lower level subcontractors. Information from line 9 and column.7 d) Initial Insurance Credit The work performed by the Subcontractor and all lower level tiers. Information obtained from line Identified Trades NOT yet assigned to a Subcontractor For each trade, not yet assigned to a Subcontractor, estimate the amount of work and insurance costs on Aon Form-1s. a) Amount of Contract The Estimated cost to subcontract the work. Information is obtained from the Proposed Contract Cost from Bid Information Section (2). b) Estimated Worker-hours The estimated on-site trade worker-hours. Information from line 9 and column 6. c) Estimated Payroll The estimated on-site trade payroll. Information from line 9 and column 7. Initial Insurance Credit the computed insurance costs for the trade based on estimated subcontract cost, including Contract Amount, Worker-hours and Payroll. The OCIP Administrator is available to provide reasonable insurance rates for computing the insurance costs on the Aon Form-1. Information obtained from line Total Estimates for Contract The total amount entered in column a, b, c, and d. 8. Composite Rate for Contract The Total Initial Insurance Credit divided by the Total Estimated Payroll (line 7d / 7c).
30 Form-3 ENROLLMENT APPLICATION (Instructions located on the following page) LAUSD Page 1 of 2 It is suggested that you examine your current Workers Compensation and General Liability Policies or contact your Insurance Agent to assist you with completing this form. *** NOTICE *** Enrollment is not automatic and requires the satisfactory completion of the Aon Form-3. In addition, you must submit a Certificate of Insurance providing evidence of your off-site coverages and automobile liability insurance. Please refer to the Insurance Manual & Safety Standards for coverage requirements. 1. Contractor Information: Federal ID No.: Company Name & dba / Contact Name & Title: Address: City, State Zip Code: Telephone: Fax: Address: Entity: Sole Proprietor Partnership u Business Information (headquarters) 2. Provide your current Workers Compensation Information: u Contact Information (address questions to ) Corporation Other: Anniversary Rating Date: Experience Modification: Bureau File Number: Your WC Insurance Carrier: Policy #: Effective Date: Expiration Date: 3. Contract Information: Contract #: Contract Description: Prime Sub Subcontractor Location of Work: Status on Project: Subcontractor Other If you are a Sub, Identify Contract Award Date: who your contract is with: Provide Payroll by Class Code in the following space provided (attach a separate sheet if necessary) State Class Code Description Worker-hours Payroll Contacts: Totals Position Name & Title Phone Fax e.mail address Project Mngr: Safety Rep: Residnt Engnr: Contract Admin: Payroll: Claims: Start Date: Actual Estimated Completion Date: Actual Estimated Contract Amount:
31 Form-3 ENROLLMENT APPLICATION (Instructions located on the following page) LAUSD Page 2 of 2 4. Subcontract Information: List any Subcontractors that will be working for you on this project (complete the information in the following table). Use additional paper if necessary: Subcontractor Address Subcontract $ Phone Contact Person 5. Will you have any off-site location(s) 100% dedicated to this project? Yes No If yes, please provide address: 6. If you are a subsidiary and/or division of another company, complete an ERM-14 Form. If you are a participant as a joint venture partner, also complete an ERM-14 form. 7. Please check if: Any aircraft will used on this project Any watercraft will used on this project 8. Does your firm participate in Alternative Dispute Resolution with the Union? Yes No WARRANTY Workers Compensation, General Liability and Excess Insurance coverages, as stated in the Contract Documents, are provided by the District. The undersigned agrees and warrants: 9. It is the Contractor s responsibility to notify it s own insurance carrier to exclude from its regular insurance all Work to be performed at the Project Site under this Contract 10. The statements in this insurance application are true to the best of my knowledge. 11. Contractor warrants that their cost of OCIP insurance and the cost of OCIP insurance for all subcontracted Work has been deducted from the bid. 12. Contractor agrees to be solely responsible for the cost of the non-ocip insurance specified in the Contract. 13. The costs of premiums for the coverage provided by the OCIP shall be paid by the District. The District will receive or pay, as the case may be, all adjustments to such costs, whether by way of dividends, retrospective rating adjustments, return premiums, audits or otherwise. Each Contractor and each of its Subcontractors shall execute any instruments of assignment as may be necessary to permit the District to receive such adjustments, unless otherwise provided in the Contract Documents. Date: Name: (please print) Title: Signature: Mail to: LAUSD OCIP Administrator Fax to: LAUSD OCIP Administrator Aon Risk Services, Inc. Aon Risk Services, Inc N. Milwaukee Ave. Fax (800) Glenview, IL Phone: (866)
32 INSTRUCTION FOR ENROLLMENT APPLICATION (AON FORM-3) This form must be completed and submitted by each Contractor and Subcontractor of any tier prior to Site mobilization for each contract awarded. The Contractor and Subcontractor will submit the completed forms to Aon Risk Services. Upon receipt of this form, Aon will issue, to the Contractor and Subcontractor, a Certificate of Insurance evidencing coverage in the Owner Controlled Insurance Program. The completed Certificate of Insurance and workers compensation insurance policy will be mailed to each Enrolled Contractor and Subcontractor. 1. Contractor Information Supply the Federal ID Number, Legal Company Name (include the doing business as, dba if applicable), mailing address and phone numbers. Identify the individual that will answer insurance questions and be responsible for your OCIP Worker s Compensation policy. Also identify the legal structure of your company by checking one of the boxes. If you choose Other, write the structure in the space provided 2. Provide your current Workers Compensation Information a) Enter information concerning your Worker s Compensation Experience Modifier in the table. Refer to your copy of the Bureau s Rating Calculation or contact your insurance agent or broker. i) The Anniversary Rating Date is the effective date of your unique Experience Modifier. Factor. ii) The Experience Modification Factor is calculated by the Rating Bureau based on your loss experience and payroll. iii) The Bureau File Number is your identification number with the Bureau. It may also be referred to as a Risk Identification Number. b) Enter information concerning your current Worker s Compensation Policy. This information is available on the Declarations or Information page. 3. Contract Information a) Provide the contract number that was assigned by the District or the party you contract with. b) Provide a brief description of your work under this contract number. c) Identify the location of your contract work. This could be an area, phase or sub-project. (Hobart Elementary is example) d) Identify your status by checking one of the boxes provided. If you select other, identify what type of a contractor you are. e) Identify the effective date of your contract. f) If you are a Subcontractor, identify with whom you have a contract. g) Contacts Communication is key to a successful OCIP. Identify the key contacts for each function listed and provide the information requested. If a single individual handles multiple job duties, be sure to list the functions that apply. h) Provide the Start Date and the Completion Date. Identify if these are the actual dates or have been estimated. i) Provide the amount of your contract. If you have a time and materials contract, provide a reasonable estimate of your anticipated activity. 4. Subcontract Information - List Subcontractors that will perform work on-site during the term of your Contract. Enrollment is NOT automatic. If you add or change subcontracting firms during the course of your contract, be sure to notify the OCIP Administrator. 5. Indicate if you have off-site location(s), including warehouses, that are dedicated to this project by checking the appropriate box. If the answer is yes, provide the address. If additional room is need, attach a separate sheet. Be sure to include the Address, City, State and Zip Code. 6. ERM-14 forms are available upon request. Please contact the OCIP Administrator. 7. Check the appropriate box if you will be using aircraft or watercraft. 8. Indicate if your company participates in Alternative Dispute Resolution with the Union. Read the Warranty statements completely. Sign the Aon Form-3 and return it to the OCIP Administrator using the information supplied at the bottom of the form. This form has been designed to fit in a standard window envelope for your convenience.
33 Form-4 ON-SITE PAYROLL REPORT (Complete a Separate Form for Each Contract with the District) LAUSD Page 1 of 1 Delay in providing this report may result in progress payments being withheld. 1. Period Beginning: Period Ending: Year: 2. Contractor: 3. Under Contract to: 4. Contract #: 5. State 6. Workers Compensation Class Code 7. Work Description 8. Worker-Hours 9. Reportable Payroll * TOTALS: *Do not include premium (excess) overtime wages; use straight time wage rates only. I VERIFY THAT THE DATA SHOWN ABOVE IS CORRECT. 10. Signed: Title: ( must be signed by an Officer of the Company) Date: CHECK IF THIS IS THE LAST PAYROLL REPORT Mail to: LAUSD OCIP Administrator or Fax to: LAUSD OCIP Administrator Aon Risk Services, Inc. Aon Risk Services, Inc N. Milwaukee Ave. Fax: (800) Glenview, IL Phone: (866)
34 INSTRUCTION FOR ON-SITE PAYROLL REPORT (AON FORM-4) This form must be completed each month by every Enrolled Contractor and Enrolled Subcontractor of any tier performing work at the Project Site (s) for each Contract awarded. The Contractor/Subcontractor must send the completed report to Aon Risk Services. Contractors will be responsible for the submission of this form by their Subcontractors. Aon Risk Services can forward a supply of these forms to your company. COMPLETION INSTRUCTIONS 1. Reporting Period - Fill in the month ending date for which this report is supplying payroll information 2. Name of Contractor/Subcontractor - Your firm s name 3. Your Contract with - The Contractor if you are a Subcontractor; your subcontractor if you are Sub- Subcontractor 4. Contract Number - Contract number of the Work you are performing 5. State Identify the State in which the work occurred. 6. Workers Compensation Classification Code Use the Classification Codes on Aon-3 form. 7. Work Description - Provide a brief description of the work. Refer to your Workers Compensation policy. 8. Worker-hours - List worker-hours for each class code. 9. Payroll List payroll for each class code for on-site work. NOTE: List only straight time/unburdened payroll (overtime as straight time). List one cumulative monthly figure for all employees who fall under each class code. 10. Signature - Please have appropriate officer of the company sign and date the completed form.
35 F ORMS Form-5 NOTICE OF WORK COMPLETION LAUSD Page 1 of 1 1. Contractor Name: 2. Contract #: 3. Description of Work: 4. Date On-Site Work Completed: 5. The following Subcontractors have completed their Work at the Site: (Add attachment if more space is needed) NAME CONTRACT # DATE ON-SITE WORK COMPLETED 6. Location of your payroll audit records: Address: Contact/Phone #: The undersigned acknowledges request for termination of coverage under the OCIP as of the date indicated above for the specified Contract. Should we return to the work Site, we will be working under our own insurance program and must provide the District with a Certificate of Insurance showing our own coverage as outlined in our contract. 7. Signed by: 8. Approved by: Title Construction Manager Date Date il to: LAUSD OCIP Administrator or Fax to: LAUSD OCIP Administrator Aon Risk Services, Inc. Aon Risk Services, Inc N. Milwaukee Ave. Fax: (800) Glenview, IL Phone: (866)
36 F ORMS INSTRUCTION FOR NOTICE OF WORK COMPLETION (AON FORM-5) This form must be completed and returned to the OCIP Administrator by the Enrolled Contractor or Enrolled Subcontractor whenever work is completed for each Contract. The Contractor will receive the final payment after all Contractor and Subcontractor information is complete. COMPLETION INSTRUCTIONS 1. Contractor Name: If you are a Subcontractor, the name of the Contractor. If you are a Sub-Subcontractor, the name of the Subcontractor. 2. Contract #: The Contract or Specification number(s) relating to the Work at the Project Site. 3. Description of Work Performed: Type of work performed under your Contract. 4. Date Work On-Site Completed: Fill in appropriate date. 5. Subcontractors of all tiers included in the Work: Names Subcontractors of all tiers associated with the close-out. 6. Final Audits Payroll Records: List name of terminating Contractor and applicable Subcontractors. 7. Signature: The Signature of the Contractor Closing-out 8. Approved by: The Signature of the District or the Construction Manager.
37 F ORMS
38 F ORMS
39 F ORMS

40 F ORMS
All written implementation materials are provided in both English and Spanish. The Employee MPN Information packet includes the following documents:
 Dear Employer, Your company has elected to participate in the Medical Provider Network (MPN) Program, which is the MPN utilized by Hanover Insurance Company for workers compensation. This letter is designed
Dear Employer, Your company has elected to participate in the Medical Provider Network (MPN) Program, which is the MPN utilized by Hanover Insurance Company for workers compensation. This letter is designed
LONG BEACH UNIFIED SCHOOL DISTRICT MEASURE K BOND PROGRAM OWNER CONTROLLED INSURANCE PROGRAM. Insurance Manual. Insurance Manual
 LONG BEACH UNIFIED SCHOOL DISTRICT MEASURE K BOND PROGRAM OWNER CONTROLLED INSURANCE PROGRAM Insurance Manual Insurance Manual 7-25-11 OWNER CONTROLLED INSURANCE PROGRAM Insurance Manual The information
LONG BEACH UNIFIED SCHOOL DISTRICT MEASURE K BOND PROGRAM OWNER CONTROLLED INSURANCE PROGRAM Insurance Manual Insurance Manual 7-25-11 OWNER CONTROLLED INSURANCE PROGRAM Insurance Manual The information
LONG BEACH UNIFIED SCHOOL DISTRICT MEASURE K BOND PROGRAM OWNER CONTROLLED INSURANCE PROGRAM. Insurance Manual. LBUSD Insurance Manual
 LONG BEACH UNIFIED SCHOOL DISTRICT MEASURE K BOND PROGRAM OWNER CONTROLLED INSURANCE PROGRAM Insurance Manual LBUSD Insurance Manual 01-25-16 OWNER CONTROLLED INSU R ANCE PROGRAM Insurance Manual The information
LONG BEACH UNIFIED SCHOOL DISTRICT MEASURE K BOND PROGRAM OWNER CONTROLLED INSURANCE PROGRAM Insurance Manual LBUSD Insurance Manual 01-25-16 OWNER CONTROLLED INSU R ANCE PROGRAM Insurance Manual The information
LOS ANGELES UNIFIED SCHOOL DISTRICT
 LOS ANGELES UNIFIED SCHOOL DISTRICT Owner Controlled Insurance Program The School Repair and Construction Program Insurance Manual Insurance Manual September 26, 2007 OCIP II Table of Contents Overview...
LOS ANGELES UNIFIED SCHOOL DISTRICT Owner Controlled Insurance Program The School Repair and Construction Program Insurance Manual Insurance Manual September 26, 2007 OCIP II Table of Contents Overview...
LOS ANGELES UNIFIED SCHOOL DISTRICT
 LOS ANGELES UNIFIED SCHOOL DISTRICT Owner Controlled Insurance Program The School Repair and Construction Program Insurance Manual Insurance Manual Version 6.0 January 5, 2009 - OCIP II Table of Contents
LOS ANGELES UNIFIED SCHOOL DISTRICT Owner Controlled Insurance Program The School Repair and Construction Program Insurance Manual Insurance Manual Version 6.0 January 5, 2009 - OCIP II Table of Contents
SIHI México, S. de R.L. de C.V. Pricing Guide
 Pricing Guide Rates effective as of: October 1, 2016 Note: Rates are subject to change without prior notice. Rates are stated in Mexican Pesos unless otherwise specified. page 1 of 5 Table Of Contents
Pricing Guide Rates effective as of: October 1, 2016 Note: Rates are subject to change without prior notice. Rates are stated in Mexican Pesos unless otherwise specified. page 1 of 5 Table Of Contents
LOS ANGELES UNIFIED SCHOOL DISTRICT
 LOS ANGELES UNIFIED SCHOOL DISTRICT Owner Controlled Insurance Program The School Repair and Construction Program Insurance Manual Insurance Manual Version 7.0 January 5, 2009 - OCIP II Table of Contents
LOS ANGELES UNIFIED SCHOOL DISTRICT Owner Controlled Insurance Program The School Repair and Construction Program Insurance Manual Insurance Manual Version 7.0 January 5, 2009 - OCIP II Table of Contents
CRAIG D JOSES P.O. BOX 416 SAN ANDREAS CA,95249
 Policy Number : P.O. BOX 416 SAN ANDREAS CA,95249 MUSA 21090_11-2010 PERSONAL AUTO POLICY DECLARATIONS CA SELECT AUTO (CA) These are your Declarations. Please Read and Attach to Your Policy. Your Producer:
Policy Number : P.O. BOX 416 SAN ANDREAS CA,95249 MUSA 21090_11-2010 PERSONAL AUTO POLICY DECLARATIONS CA SELECT AUTO (CA) These are your Declarations. Please Read and Attach to Your Policy. Your Producer:
Sentry Insurance Group 1800 North Point Drive, Stevens Point, WI
 Sentry Insurance Group 1800 North Point Drive, Stevens Point, WI 54481 1-800-739-3344 WC-80-10-0001 (Ed. 7/06) 10-06 Sentry Insurance Group 1800 North Point Drive, Stevens Point, WI 54481 1-800-739-3344
Sentry Insurance Group 1800 North Point Drive, Stevens Point, WI 54481 1-800-739-3344 WC-80-10-0001 (Ed. 7/06) 10-06 Sentry Insurance Group 1800 North Point Drive, Stevens Point, WI 54481 1-800-739-3344
Favor de cortar y mantenga esta página junto con nuestra información de contacto que aparece abajo. Gracias!
 Please tear off and keep this page with our contact information below. Thank you! DEPARTMENT OF JUSTICE CRIME VICTIMS SERVICES DIVISION APPLICATION FOR CRIME VICTIM COMPENSATION You may qualify for help
Please tear off and keep this page with our contact information below. Thank you! DEPARTMENT OF JUSTICE CRIME VICTIMS SERVICES DIVISION APPLICATION FOR CRIME VICTIM COMPENSATION You may qualify for help
Workplace Safety - The Role of Staff
 The Occupational Safety and Health Act (OSHA) The Act requires each worker to comply with occupational safety and health standards, as well as all rules, regulations, and orders issued under the Act that
The Occupational Safety and Health Act (OSHA) The Act requires each worker to comply with occupational safety and health standards, as well as all rules, regulations, and orders issued under the Act that
Workers Compensation Premium Credits to Reflect 2017 Reforms
 New York Compensation Insurance Rating Board 733 Third Avenue New York, NY 10017 Tel: (212) 697 3535 July 28, 2017 R.C. 2439 Re: Workers Compensation Premium Credits to Reflect 2017 Reforms Members of
New York Compensation Insurance Rating Board 733 Third Avenue New York, NY 10017 Tel: (212) 697 3535 July 28, 2017 R.C. 2439 Re: Workers Compensation Premium Credits to Reflect 2017 Reforms Members of
Civil Rights Complaint Form
 Civil Rights Complaint Form Title VI of the 1964 Civil Rights Act and related non-discrimination statutes and regulations require that no person in the United States shall, on the ground of race, color,
Civil Rights Complaint Form Title VI of the 1964 Civil Rights Act and related non-discrimination statutes and regulations require that no person in the United States shall, on the ground of race, color,
FAMILY INDEPENDENCE ADMINISTRATION James K. Whelan, Executive Deputy Commissioner
 FAMILY INDEPENDENCE ADMINISTRATION James K. Whelan, Executive Deputy Commissioner Stephen Fisher, Assistant Deputy Commissioner Office of Procedures POLICY BULLETIN #14-100-OPE STORAGE FEE NOTICES September
FAMILY INDEPENDENCE ADMINISTRATION James K. Whelan, Executive Deputy Commissioner Stephen Fisher, Assistant Deputy Commissioner Office of Procedures POLICY BULLETIN #14-100-OPE STORAGE FEE NOTICES September
OFFICE OF POLICY, PROCEDURES, AND TRAINING James K. Whelan, Executive Deputy Commissioner
 OFFICE OF POLICY, PROCEDURES, AND TRAINING James K. Whelan, Executive Deputy Commissioner Stephen Fisher, Assistant Deputy Commissioner Office of Procedures POLICY BULLETIN #15-99-OPE ANNOUNCEMENT OF TWO
OFFICE OF POLICY, PROCEDURES, AND TRAINING James K. Whelan, Executive Deputy Commissioner Stephen Fisher, Assistant Deputy Commissioner Office of Procedures POLICY BULLETIN #15-99-OPE ANNOUNCEMENT OF TWO
EN United in diversity EN A8-0204/83. Amendment
 27.6.2018 A8-0204/83 83 Recital 2 (2) So far, and unless otherwise provided for in national law, the rules on access to the occupation of road transport operator do not apply to undertakings engaged in
27.6.2018 A8-0204/83 83 Recital 2 (2) So far, and unless otherwise provided for in national law, the rules on access to the occupation of road transport operator do not apply to undertakings engaged in
IMPORTANT. Vehicle Accident Report Kit. Another Safety Service from CNA. Keep This Kit in Your Vehicle. Contains Instructions and Forms:
 Vehicle Accident Report Kit Another Safety Service from CNA Keep This Kit in Your Vehicle Contains Instructions and Forms: Driver s Report of Motor Vehicle Accident Traffic Accident Exchange Information
Vehicle Accident Report Kit Another Safety Service from CNA Keep This Kit in Your Vehicle Contains Instructions and Forms: Driver s Report of Motor Vehicle Accident Traffic Accident Exchange Information
Employee s Injury Report / Informe de lesión de empleado
 Claims Administrative Services Phone: 800-765-2412 Fax: 903-509-1888 501 Shelley Drive Claims Administrative Services, Inc. Tyler, Texas 75701 Our reputation for excellence is no accident. / Nuestro prestigio
Claims Administrative Services Phone: 800-765-2412 Fax: 903-509-1888 501 Shelley Drive Claims Administrative Services, Inc. Tyler, Texas 75701 Our reputation for excellence is no accident. / Nuestro prestigio
Civil Rights Complaint Form
 Civil Rights Complaint Form It is the policy of the Greater Derry Salem Cooperative Alliance for Regional Transportation (CART) to uphold and assure full compliance with Title VI of the Civil Rights Act
Civil Rights Complaint Form It is the policy of the Greater Derry Salem Cooperative Alliance for Regional Transportation (CART) to uphold and assure full compliance with Title VI of the Civil Rights Act
!!!!!!!!! Dear Applicant,
 Dear Applicant, After a criminal background check was performed, is considering rescinding our offer of employment for the position of. See the attached copy of the Individualized Assessment for a more
Dear Applicant, After a criminal background check was performed, is considering rescinding our offer of employment for the position of. See the attached copy of the Individualized Assessment for a more
WORKERS COMPENSATION BASIC CLAIMS REPORTING GUIDELINES
 WORKERS COMPENSATION BASIC CLAIMS REPORTING GUIDELINES Email the completed form to Carol.Lafever@hubinternational.com or fax to (818) 257-6712. If you need more information, please email hr@srprodsvc.com
WORKERS COMPENSATION BASIC CLAIMS REPORTING GUIDELINES Email the completed form to Carol.Lafever@hubinternational.com or fax to (818) 257-6712. If you need more information, please email hr@srprodsvc.com
Verification Worksheet V4 D I
 Last Name: First Name: ID: (print clearly) 2018 2019 Verification Worksheet V4 D I Before your financial aid for the 2018/2019 award year can be finalized, federal regulations require that certain data
Last Name: First Name: ID: (print clearly) 2018 2019 Verification Worksheet V4 D I Before your financial aid for the 2018/2019 award year can be finalized, federal regulations require that certain data
entidad mexicana de acreditación, a. c.
 MUESTREO DEL PROCESO DE EVALUACIÓN DE UNIDADES DE VERIFICACIÓN (ORGANISMOS DE INSPECCIÓN) ASUNTO: En este documento se describe la forma de realizar el Muestreo para el proceso de evaluación de Unidades
MUESTREO DEL PROCESO DE EVALUACIÓN DE UNIDADES DE VERIFICACIÓN (ORGANISMOS DE INSPECCIÓN) ASUNTO: En este documento se describe la forma de realizar el Muestreo para el proceso de evaluación de Unidades
Barbara Quaid. March 1, Dear Ventura County Teachers:
 March 1, 2018 Dear Ventura County Teachers: The Ventura County Fair invites students to earn free carnival rides through our reading program, Read & Ride for local kindergarten through 8 th grade students.
March 1, 2018 Dear Ventura County Teachers: The Ventura County Fair invites students to earn free carnival rides through our reading program, Read & Ride for local kindergarten through 8 th grade students.
FAMILY INDEPENDENCE ADMINISTRATION Matthew Brune, Executive Deputy Commissioner
 FAMILY INDEPENDENCE ADMINISTRATION Matthew Brune, Executive Deputy Commissioner James K. Whelan, Deputy Commissioner Policies, Procedures, and Training POLICY BULLETIN #10-104-OPE NEW ENTRANCE TO THE EAST
FAMILY INDEPENDENCE ADMINISTRATION Matthew Brune, Executive Deputy Commissioner James K. Whelan, Deputy Commissioner Policies, Procedures, and Training POLICY BULLETIN #10-104-OPE NEW ENTRANCE TO THE EAST
Sample Parental Consent Letters
 Sample Parental Consent Letters 2015-16 The following links provide sample parental consent letters that clients are welcome to edit for their own purposes. Under applicable federal, state, and local laws,
Sample Parental Consent Letters 2015-16 The following links provide sample parental consent letters that clients are welcome to edit for their own purposes. Under applicable federal, state, and local laws,
INSTRUCCIONES. Pedimos que lea la siguiente información antes de rellenar el afidávit adjunto:
 OFFICE OF THE ATTORNEY GENERAL Citizen Services PAM BONDI ATTORNEY GENERAL STATE OF FLORIDA PL-01 The Capitol Tallahassee, FL 32399-1050 Phone (850) 414-3990 Fax (850) 410-1630 http://www.myfloridalegal.com
OFFICE OF THE ATTORNEY GENERAL Citizen Services PAM BONDI ATTORNEY GENERAL STATE OF FLORIDA PL-01 The Capitol Tallahassee, FL 32399-1050 Phone (850) 414-3990 Fax (850) 410-1630 http://www.myfloridalegal.com
Going Home. Medicines. Pain. Diet
 Going Home After an illness or injury, some things may change in your life. Make sure you and your family know the answers to these questions before you go home from the hospital. Medicines Am I taking
Going Home After an illness or injury, some things may change in your life. Make sure you and your family know the answers to these questions before you go home from the hospital. Medicines Am I taking
Part No: KTI (Page 1-13) (Pagina 14-26) K-Tool International Wixom, MI 48393
 (Pagina 14-26) K-Tool International Wixom, MI 48393") Part No: KTI-70099 (Page 1-13) (Pagina 14-26) K-Tool International Wixom, MI 48393 (800) 762-6002 www.ktoolinternational.com support@ktoolinternational.com The KTool Walkie-Talkie can use a NiMH rechargeable
Part No: KTI-70099 (Page 1-13) (Pagina 14-26) K-Tool International Wixom, MI 48393 (800) 762-6002 www.ktoolinternational.com support@ktoolinternational.com The KTool Walkie-Talkie can use a NiMH rechargeable
Employer Employer Address Phone. Phone: Home Work Cell
 PATIENT REGISTRATION Last Name First Name MI Date of Birth Age Social Security # Gender Marital Status Address Street Apt# City State Zip Phone: Home Work Cell E-Mail Occupation Retired: Yes No Employer
PATIENT REGISTRATION Last Name First Name MI Date of Birth Age Social Security # Gender Marital Status Address Street Apt# City State Zip Phone: Home Work Cell E-Mail Occupation Retired: Yes No Employer
Notice to Employees. Your employer is insured under the Workers Compensation Act by Pinnacol Assurance.
 Workers Compensation Act Notice to Employees Your employer is insured under the Workers Compensation Act by Pinnacol Assurance. If you are injured or sustain an occupational disease while at work, you
Workers Compensation Act Notice to Employees Your employer is insured under the Workers Compensation Act by Pinnacol Assurance. If you are injured or sustain an occupational disease while at work, you
For more information regarding these forms please go to the Texas Department of Insurance website http://www.tdi.state.tx.us/forms/form20employer.
 CAPROCK Claims Management, LLC ROCK SOLID PERFORMANCE AND RESULTS PO Box 743427 Dallas, TX 75374 (888) 812-3577 Fax (972) 934-3091 IMPORTANT NOTICE FOR REQUIRED FILING FORMS DWC FORM-5 & DWC FORM-7 Caprock
CAPROCK Claims Management, LLC ROCK SOLID PERFORMANCE AND RESULTS PO Box 743427 Dallas, TX 75374 (888) 812-3577 Fax (972) 934-3091 IMPORTANT NOTICE FOR REQUIRED FILING FORMS DWC FORM-5 & DWC FORM-7 Caprock
Encl.: Teacher/Teacher Assistant Information Request Form
 To: All Parents/Legal Guardians in Title I Schools From: Charlotte-Mecklenburg Schools Title I Department Date: September 27, 2017 Subject: Right to Know Notification to Parents of Teacher and Teacher
To: All Parents/Legal Guardians in Title I Schools From: Charlotte-Mecklenburg Schools Title I Department Date: September 27, 2017 Subject: Right to Know Notification to Parents of Teacher and Teacher
Workers Compensation Non-Subscriber Form
 Workers Compensation Non-Subscriber Form Texas is unique in one very important respect: It s the only state in which employers have the choice to carry workers compensation insurance or not. There are
Workers Compensation Non-Subscriber Form Texas is unique in one very important respect: It s the only state in which employers have the choice to carry workers compensation insurance or not. There are
2770 South Taylor Street Arlington, Virginia Phone: (703) STUDENT ATHLETE ACCIDENT INSURANCE COVERAGE
 STUDENT ATHLETE ACCIDENT INSURANCE COVERAGE") Arlington Public Schools FACILITIES AND OPERATIONS September 5, 2017 2770 South Taylor Street Arlington, Virginia 22206 Phone: (703) 228-7740 STUDENT ATHLETE ACCIDENT INSURANCE COVERAGE Dear Parent/Guardian,
Arlington Public Schools FACILITIES AND OPERATIONS September 5, 2017 2770 South Taylor Street Arlington, Virginia 22206 Phone: (703) 228-7740 STUDENT ATHLETE ACCIDENT INSURANCE COVERAGE Dear Parent/Guardian,
News Flash! Primary & Specialty Care Providers. Sharp Health Plan. Date: February 17, 2012. Subject: Member Grievance Forms
 I M P O R T A N T News Flash! A FAX Publication for Providers of Sharp Health Plan To: From: Primary & Specialty Care Providers Sharp Health Plan Date: February 17, 2012 Subject: Member Grievance Forms
I M P O R T A N T News Flash! A FAX Publication for Providers of Sharp Health Plan To: From: Primary & Specialty Care Providers Sharp Health Plan Date: February 17, 2012 Subject: Member Grievance Forms
MASSACHUSETTS LABORERS PENSION FUND
 MASSACHUSETTS LABORERS PENSION FUND 14 New England Executive Park Suite 200 Burlington, Massachusetts 01803-5201 Telephone (781) 272-1000 Toll Free (800) 342-3792 Fax (781) 272-2226 Haga Clic Aquí Para
MASSACHUSETTS LABORERS PENSION FUND 14 New England Executive Park Suite 200 Burlington, Massachusetts 01803-5201 Telephone (781) 272-1000 Toll Free (800) 342-3792 Fax (781) 272-2226 Haga Clic Aquí Para
I, the. submits the. The Annual Guardianship Plan for the period beginning, El Informe anual de la tutela corresponde al periodo que se inicia el
 IN THE CIRCUIT COURT FOR ORANGE COUNTY, FLORIDA PROBATE DIVISION / DIVISIÓN DE SUCESIONES IN RE: GUARDIAN ADVOCATE OF ASUNTO: CURADOR DE Case No /No. de causa: ANNUAL GUARDIAN ADVOCATE REPORT ANNUAL GUARDIAN
IN THE CIRCUIT COURT FOR ORANGE COUNTY, FLORIDA PROBATE DIVISION / DIVISIÓN DE SUCESIONES IN RE: GUARDIAN ADVOCATE OF ASUNTO: CURADOR DE Case No /No. de causa: ANNUAL GUARDIAN ADVOCATE REPORT ANNUAL GUARDIAN
Ada County Existing/Resale
 Ada County Existing/Resale tember 2018 ket Statistics Report provided by Boise Regional REALTORS Key Metrics 2017 2018 % Chg YTD 2017 YTD 2018 % Chg Closed Sales 811 616-24.0% 6,301 6,136-2.6% Median Sales
Ada County Existing/Resale tember 2018 ket Statistics Report provided by Boise Regional REALTORS Key Metrics 2017 2018 % Chg YTD 2017 YTD 2018 % Chg Closed Sales 811 616-24.0% 6,301 6,136-2.6% Median Sales
For Parents and Caregivers
 Who Qualifies How to Enroll WHO QUALIFIES FOR WIC: HOW TO ENROLL IN WIC: You must Bring the infant or child to the WIC office to complete initial enrollment. If the infant or child can t be there because
Who Qualifies How to Enroll WHO QUALIFIES FOR WIC: HOW TO ENROLL IN WIC: You must Bring the infant or child to the WIC office to complete initial enrollment. If the infant or child can t be there because
aviación AIRPORT LEGAL LIABILITY RESPONSABILIDAD LEGAL DE AUEROPUERTOS Name and address of Insured and Name of Airport(s).
.") Name and address of Insured and Name of Airport(s). 1. Nombre y dirección del Asegurado y Nombre de el(los) Aeropuerto(s). Is the Insured the owner and/or operator of the Airport(s)? 2. Es el Asegurado
Name and address of Insured and Name of Airport(s). 1. Nombre y dirección del Asegurado y Nombre de el(los) Aeropuerto(s). Is the Insured the owner and/or operator of the Airport(s)? 2. Es el Asegurado
Ada County Existing/Resale
 Ada County Existing/Resale October 2018 ket Statistics Report provided by Boise Regional REALTORS Data from the Intermountain MLS as of ember 11, 2018 Key Metrics Oct 2017 Oct 2018 % Chg YTD 2017 YTD 2018
Ada County Existing/Resale October 2018 ket Statistics Report provided by Boise Regional REALTORS Data from the Intermountain MLS as of ember 11, 2018 Key Metrics Oct 2017 Oct 2018 % Chg YTD 2017 YTD 2018
Action Required by September 30, 2018 in order to Participate as a Provider in the Puerto Rico Medicaid Government Health Plan Program
 CIRCULAR LETTER #M1807134 September 15, 2018 Action Required by September 30, 2018 in order to Participate as a Provider in the Puerto Rico Medicaid Government Health Plan Program Dear Provider, Greetings
CIRCULAR LETTER #M1807134 September 15, 2018 Action Required by September 30, 2018 in order to Participate as a Provider in the Puerto Rico Medicaid Government Health Plan Program Dear Provider, Greetings
2 DATOS DE LA EMPRESA O PROFESIONAL / COMPANY OR PROFESSIONAL'S DETAILS. Dirección de correo electrónico: Telephone number. Electronic address
 Sevilla, 27 de marzo 2008 BOJA núm. 60 Página núm. 13 ANEXO I. MODELO DE HOJAS DE QUEJAS Y RECLAMACIONES. ANVERSO JUNTA DE ANDALUCIA CONSEJERÍA DE GOBERNACIÓN HOJA DE QUEJAS Y RECLAMACIONES / COMPLAINTS
Sevilla, 27 de marzo 2008 BOJA núm. 60 Página núm. 13 ANEXO I. MODELO DE HOJAS DE QUEJAS Y RECLAMACIONES. ANVERSO JUNTA DE ANDALUCIA CONSEJERÍA DE GOBERNACIÓN HOJA DE QUEJAS Y RECLAMACIONES / COMPLAINTS
Canyon County Existing/Resale
 Canyon County Existing/Resale tember 2018 ket Statistics Key Metrics 2017 2018 % Chg YTD 2017 YTD 2018 % Chg Closed Sales 366 301 17.8% 2,803 2,953 5.4% Median Sales Price $176,000 $210, 19.6% $170,000
Canyon County Existing/Resale tember 2018 ket Statistics Key Metrics 2017 2018 % Chg YTD 2017 YTD 2018 % Chg Closed Sales 366 301 17.8% 2,803 2,953 5.4% Median Sales Price $176,000 $210, 19.6% $170,000
IE12_ CONSOLIDACIÓN Y DESARROLLO DE NUEVAS TÉCNICAS DE EVALUACIÓN INTENSIVAS ON-LINE YA IMPLEMENTADAS POR EL GIE E4
 IE12_13-03001 - CONSOLIDACIÓN Y DESARROLLO DE NUEVAS TÉCNICAS DE EVALUACIÓN Departamento de Estructuras de la Edificación Escuela Técnica Superior de Arquitectura de Madrid Universidad Politécnica de Madrid
IE12_13-03001 - CONSOLIDACIÓN Y DESARROLLO DE NUEVAS TÉCNICAS DE EVALUACIÓN Departamento de Estructuras de la Edificación Escuela Técnica Superior de Arquitectura de Madrid Universidad Politécnica de Madrid
SAMPLE. Person ID Number:
 NYS OTDA STATE SUPPLEMENT PROGRAM PO BOX 1740 ALBANY, NEW YORK 12201 New York State Office of Temporary and Disability Assistance John Q Public 123 Main Street Any Town, NY 12345 SAMPLE Person ID Number:
NYS OTDA STATE SUPPLEMENT PROGRAM PO BOX 1740 ALBANY, NEW YORK 12201 New York State Office of Temporary and Disability Assistance John Q Public 123 Main Street Any Town, NY 12345 SAMPLE Person ID Number:
Canyon County Existing/Resale
 Canyon County Existing/Resale October 2018 ket Statistics Data from the Intermountain MLS as of ember 11, 2018 Key Metrics Oct 2017 Oct 2018 % Chg YTD 2017 YTD 2018 % Chg Closed Sales 331 349 5.4% 3,134
Canyon County Existing/Resale October 2018 ket Statistics Data from the Intermountain MLS as of ember 11, 2018 Key Metrics Oct 2017 Oct 2018 % Chg YTD 2017 YTD 2018 % Chg Closed Sales 331 349 5.4% 3,134
AUTHORIZATION FOR USE OR DISCLOSURE OF HEALTH INFORMATION
 FORM 16-1 AUTHORIZATION FOR USE OR DISCLOSURE OF HEALTH INFORMATION Completion of this document authorizes the disclosure and use of health information about you. Failure to provide all information requested
FORM 16-1 AUTHORIZATION FOR USE OR DISCLOSURE OF HEALTH INFORMATION Completion of this document authorizes the disclosure and use of health information about you. Failure to provide all information requested
Triple-S Salud, Inc. is an independent licensee of BlueCross BlueShield Association.
 Circular Letter#M1807112 August 1, 2018 Action Required by September 15, 2018 in Order to Participate as a Provider in the Puerto Rico Medicaid Government Health Plan Program Dear Provider: Due to a recent
Circular Letter#M1807112 August 1, 2018 Action Required by September 15, 2018 in Order to Participate as a Provider in the Puerto Rico Medicaid Government Health Plan Program Dear Provider: Due to a recent
Authorization for Use or Disclosure of
 F o r m 1 6-1 Authorization for Use or Disclosure of Health Information Completion of this document authorizes the disclosure and use of health information about you. Failure to provide all information
F o r m 1 6-1 Authorization for Use or Disclosure of Health Information Completion of this document authorizes the disclosure and use of health information about you. Failure to provide all information
Informacion Basica de el paciente
 Informacion Basica de el paciente Cash Fecha: Apellido: Nombre: Inicial: Direccion: Pueblo: Estado: Zip: Telefono de la casa o celular: Telefono del trabajo: Numero de seguro social: Fecha de nacimiento:
Informacion Basica de el paciente Cash Fecha: Apellido: Nombre: Inicial: Direccion: Pueblo: Estado: Zip: Telefono de la casa o celular: Telefono del trabajo: Numero de seguro social: Fecha de nacimiento:
FAMILY INDEPENDENCE ADMINISTRATION Seth W. Diamond, Executive Deputy Commissioner
 FAMILY INDEPENDENCE ADMINISTRATION Seth W. Diamond, Executive Deputy Commissioner James K. Whelan, Deputy Commissioner Policy, Procedures and Training Lisa C. Fitzpatrick, Assistant Deputy Commissioner
FAMILY INDEPENDENCE ADMINISTRATION Seth W. Diamond, Executive Deputy Commissioner James K. Whelan, Deputy Commissioner Policy, Procedures and Training Lisa C. Fitzpatrick, Assistant Deputy Commissioner
Section 6621 of the Internal Revenue Code establishes the interest rates on
 Part 1 Section 6621.--Determination of Rate of Interest 26 CFR 301.6621-1: Interest rate. Rev. Rul. 2014-29 Section 6621 of the Internal Revenue Code establishes the interest rates on overpayments and
Part 1 Section 6621.--Determination of Rate of Interest 26 CFR 301.6621-1: Interest rate. Rev. Rul. 2014-29 Section 6621 of the Internal Revenue Code establishes the interest rates on overpayments and
Evidence of Auto Insurance
 Evidence of Auto Insurance Insured: If this address is incorrect, Please call 1-800-999-5094 Master Policyholder/Dealership: Printed: Initial Coverage Period: From: To: *Continuation Coverage Period: From:
Evidence of Auto Insurance Insured: If this address is incorrect, Please call 1-800-999-5094 Master Policyholder/Dealership: Printed: Initial Coverage Period: From: To: *Continuation Coverage Period: From:
City of Silverton Title VI Complaint Procedures. Ciudad de Silverton Procedimientos de Quejas del Título VI
 City of Silverton Title VI Complaint Procedures Ciudad de Silverton Procedimientos de Quejas del Título VI Any person who believes she or he has been discriminated against on the basis of race, color,
City of Silverton Title VI Complaint Procedures Ciudad de Silverton Procedimientos de Quejas del Título VI Any person who believes she or he has been discriminated against on the basis of race, color,
(No. 96) (Approved September 10, 2009) AN ACT
 (Approved September 10, 2009) AN ACT") (S. B. 876) (No. 96) (Approved September 10, 2009) AN ACT To amend Sections 9-304(1) and 9-308(a) of Chapter 9 of Act No. 208 of August 17, 1995, as amended, known as the Negotiable Instruments and Banking
(S. B. 876) (No. 96) (Approved September 10, 2009) AN ACT To amend Sections 9-304(1) and 9-308(a) of Chapter 9 of Act No. 208 of August 17, 1995, as amended, known as the Negotiable Instruments and Banking
Township of Union Complaint Form. Note: The following information is needed to assist in processing your complaint.
 Township of Union Complaint Form Note: The following information is needed to assist in processing your complaint. A. Complainant s information: Name: Address: City/State/Zip Code: Telephone Number (Home):
Township of Union Complaint Form Note: The following information is needed to assist in processing your complaint. A. Complainant s information: Name: Address: City/State/Zip Code: Telephone Number (Home):
LONG BEACH UNIFIED SCHOOL DISTRICT
 LONG BEACH UNIFIED SCHOOL DISTRICT Parent/Guardian Complaint Concerning District Personnel Pursuant to Education Code Section 35160.5, the District has a carefully defined procedure for processing complaints
LONG BEACH UNIFIED SCHOOL DISTRICT Parent/Guardian Complaint Concerning District Personnel Pursuant to Education Code Section 35160.5, the District has a carefully defined procedure for processing complaints
MYCHART PROXY ACCESS INFORMATION PAGE PÁGINA DE INFORMACIÓN PARA EL ACCESO DE REPRESENTANTE A MYCHART
 FORMULARIO PARA EL ACCESSO DE REPRESENTANTE A MYCHART MYCHART PROXY ACCESS INFORMATION PAGE PÁGINA DE INFORMACIÓN PARA EL WHAT IS PROXY ACCESS? QUÉ ES UN ACCESO DE REPRESENTANTE? MyChart Proxy Access allows
FORMULARIO PARA EL ACCESSO DE REPRESENTANTE A MYCHART MYCHART PROXY ACCESS INFORMATION PAGE PÁGINA DE INFORMACIÓN PARA EL WHAT IS PROXY ACCESS? QUÉ ES UN ACCESO DE REPRESENTANTE? MyChart Proxy Access allows
PRODUCT OBSOLESCENCE NOTICE August 31, 2013
 PRODUCT OBSOLESCENCE NOTICE August 31, 2013 Dear Customer, Murata Power Solutions hereby gives official notification that the products listed in this Notice are being rendered Obsolete. We are offering
PRODUCT OBSOLESCENCE NOTICE August 31, 2013 Dear Customer, Murata Power Solutions hereby gives official notification that the products listed in this Notice are being rendered Obsolete. We are offering
GENEX SERVICES, LLC GENEX
 Continuity of Care Policy This attachment contains the MPN Applicant s written policy for Continuity of Care to an injured covered employee with a provider whose membership in the Genex MPN has been terminated.
Continuity of Care Policy This attachment contains the MPN Applicant s written policy for Continuity of Care to an injured covered employee with a provider whose membership in the Genex MPN has been terminated.
Workers Compensation Packet
 MIDLAND INDEPENDENT SCHOOL DISTRICT BENEFITS DEPT. / 615 W. MISSOURI STE 720 / MIDLAND, TX 79701 (432) 240-1950 Workers Compensation Packet For the Injured Employee Attached are three forms that must be
MIDLAND INDEPENDENT SCHOOL DISTRICT BENEFITS DEPT. / 615 W. MISSOURI STE 720 / MIDLAND, TX 79701 (432) 240-1950 Workers Compensation Packet For the Injured Employee Attached are three forms that must be
Florida Department of Transportation Title VI Complaint Procedure
 FTA Circular 4702.1B, Chapter III, Paragraph 6: All recipients shall develop procedures for investigating and tracking Title VI complaints filed aginst them and make their procedures for filing a complaint
FTA Circular 4702.1B, Chapter III, Paragraph 6: All recipients shall develop procedures for investigating and tracking Title VI complaints filed aginst them and make their procedures for filing a complaint
Guide to Health Insurance Part II: How to access your benefits and services.
 Guide to Health Insurance Part II: How to access your benefits and services. 1. I applied for health insurance, now what? Medi-Cal Applicants If you applied for Medi-Cal it will take up to 45 days to find
Guide to Health Insurance Part II: How to access your benefits and services. 1. I applied for health insurance, now what? Medi-Cal Applicants If you applied for Medi-Cal it will take up to 45 days to find
This Employer Participates in E-Verify
 This Employer Participates in E-Verify This employer will provide the Social Security Administration (SSA) and, if necessary, the Department of Homeland Security (DHS), with information from each new employee
This Employer Participates in E-Verify This employer will provide the Social Security Administration (SSA) and, if necessary, the Department of Homeland Security (DHS), with information from each new employee
INTERNATIONAL ADMISSIONS
 INTERNATIONAL ADMISSIONS ADMISIONES INTERNACIONALES IMPORTANT: ENTIRE APPLICATION MUST BE COMPLETED. PLEASE READ CAREFULLY. IMPORTANTE: SE DEBE COMPLETAR TODA LA SOLICITUD. FAVOR DE LEER CON DETENIMIENTO.
INTERNATIONAL ADMISSIONS ADMISIONES INTERNACIONALES IMPORTANT: ENTIRE APPLICATION MUST BE COMPLETED. PLEASE READ CAREFULLY. IMPORTANTE: SE DEBE COMPLETAR TODA LA SOLICITUD. FAVOR DE LEER CON DETENIMIENTO.
EULA LEE CARTER MEMORIAL FUND
 EULA LEE CARTER MEMORIAL FUND GUIDELINES AND APPLICATION Applicants/Recipients 1. Applicants shall have been members of Delta Kappa Gamma chapters in Latin American countries in the Southwest Region for
EULA LEE CARTER MEMORIAL FUND GUIDELINES AND APPLICATION Applicants/Recipients 1. Applicants shall have been members of Delta Kappa Gamma chapters in Latin American countries in the Southwest Region for
Workers' Compensation fraud and abuse divert District money that could be used for other purposes such as textbooks, supplies, salaries, etc.
 Overview Workers' Compensation fraud and abuse divert District money that could be used for other purposes such as textbooks, supplies, salaries, etc. It is unlawful to make any knowingly false or fraudulent
Overview Workers' Compensation fraud and abuse divert District money that could be used for other purposes such as textbooks, supplies, salaries, etc. It is unlawful to make any knowingly false or fraudulent
VERIFICATION WORKSHEET V4 custom VERIFICATION GROUP
 2017-2018 VERIFICATION WORKSHEET V4 custom VERIFICATION GROUP We ve reviewed your 2017 2018 Free Application for Federal Student Aid (FAFSA) and your application was selected for a review process called
2017-2018 VERIFICATION WORKSHEET V4 custom VERIFICATION GROUP We ve reviewed your 2017 2018 Free Application for Federal Student Aid (FAFSA) and your application was selected for a review process called
Phelan Language Academy DUAL LANGUAGE IMMERSION Providing a World of opportunities for students DUAL LANGUAGE IMMERSION APPLICATION FORM
 Phelan Language Academy DUAL LANGUAGE IMMERSION Providing a World of opportunities for students DUAL LANGUAGE IMMERSION APPLICATION FORM PLEASE NOTE: Applications need to be received by the due date and
Phelan Language Academy DUAL LANGUAGE IMMERSION Providing a World of opportunities for students DUAL LANGUAGE IMMERSION APPLICATION FORM PLEASE NOTE: Applications need to be received by the due date and
HOMEWORK ASSIGNMENTS, TEST AND QUIZ DUE DATES: STUDY GUIDE and CLASS NOTES. NOV-04 TO NOV-22, 2016 SPANISH 1 PERIOD 6 S. DePastino
 HOMEWORK ASSIGNMENTS, TEST AND QUIZ DUE DATES: STUDY GUIDE and CLASS NOTES NOV-04 TO NOV-22, 2016 SPANISH 1 PERIOD 6 S. DePastino Unidad 2 Etapa 2 11-04 A TAREA: Estudiar el vocabulario libro p. 143 Iniciar
HOMEWORK ASSIGNMENTS, TEST AND QUIZ DUE DATES: STUDY GUIDE and CLASS NOTES NOV-04 TO NOV-22, 2016 SPANISH 1 PERIOD 6 S. DePastino Unidad 2 Etapa 2 11-04 A TAREA: Estudiar el vocabulario libro p. 143 Iniciar
FERRIS INDEPENDENT SCHOOL DISTRICT NONRESIDENT STUDENT REQUEST TO TRANSFER INTO THE DISTRICT SCHOOL YEAR
 FERRIS INDEPENDENT SCHOOL DISTRICT NRESIDENT STUDENT REQUEST TO TRANSFER INTO THE DISTRICT SCHOOL YEAR 2018-2019 1. STUDENT S NAME: 2. CURRENT ADDRESS: 3. SCHOOL DISTRICT IN WHICH THE STUDENT RESIDES:
FERRIS INDEPENDENT SCHOOL DISTRICT NRESIDENT STUDENT REQUEST TO TRANSFER INTO THE DISTRICT SCHOOL YEAR 2018-2019 1. STUDENT S NAME: 2. CURRENT ADDRESS: 3. SCHOOL DISTRICT IN WHICH THE STUDENT RESIDES:
Flash News. Flash News / Septiembre 2015
 Flash News / Septiembre 2015 Flash News 11 de septiembre de 2015 Presentación de Formularios de Remesas para la aplicación de los Tratados para evitar la Doble Imposición Fiscal suscritos por la República
Flash News / Septiembre 2015 Flash News 11 de septiembre de 2015 Presentación de Formularios de Remesas para la aplicación de los Tratados para evitar la Doble Imposición Fiscal suscritos por la República
SECTION SD. HEALTH SERVICES
 SECTION SD. HEALTH SERVICES Note: Only Next-of-Kin Interviews (n=1,209). Some questions may have missing values if the section was not completed. Only n=7 observations were included in the final data sets
SECTION SD. HEALTH SERVICES Note: Only Next-of-Kin Interviews (n=1,209). Some questions may have missing values if the section was not completed. Only n=7 observations were included in the final data sets
MANUAL DE FARMACIA CLINICA Y ATENCION FARMACEUTICA. EL PRECIO ES EN DOLARES BY JOAQUIN HERRERA CARRANZA
 MANUAL DE FARMACIA CLINICA Y ATENCION FARMACEUTICA. EL PRECIO ES EN DOLARES BY JOAQUIN HERRERA CARRANZA DOWNLOAD EBOOK : MANUAL DE FARMACIA CLINICA Y ATENCION HERRERA CARRANZA PDF Click link bellow and
MANUAL DE FARMACIA CLINICA Y ATENCION FARMACEUTICA. EL PRECIO ES EN DOLARES BY JOAQUIN HERRERA CARRANZA DOWNLOAD EBOOK : MANUAL DE FARMACIA CLINICA Y ATENCION HERRERA CARRANZA PDF Click link bellow and
REPORT ON THE RESERVE FUND OF THE REGIONAL CONFERENCE ON MIGRATION FOR THE ASSISTED VOLUNTARY RETURN OF HIGHLY VULNERABLE INTRA-REGIONAL MIGRANTS
 REPORT ON THE RESERVE FUND OF THE REGIONAL CONFERENCE ON MIGRATION FOR THE ASSISTED VOLUNTARY RETURN OF HIGHLY VULNERABLE INTRA-REGIONAL MIGRANTS International Organization for Migration Salvador Gutiérrez
REPORT ON THE RESERVE FUND OF THE REGIONAL CONFERENCE ON MIGRATION FOR THE ASSISTED VOLUNTARY RETURN OF HIGHLY VULNERABLE INTRA-REGIONAL MIGRANTS International Organization for Migration Salvador Gutiérrez
Documentation of Public Hearing Opportunity
 Documentation of Public Hearing Opportunity Project Location Comal and Guadalupe Counties Farm-to-Market (FM) 1103 CSJs: 1268-01-013 and 1268-02-027 Project Limits From Interstate Highway 35 (I-35) to
Documentation of Public Hearing Opportunity Project Location Comal and Guadalupe Counties Farm-to-Market (FM) 1103 CSJs: 1268-01-013 and 1268-02-027 Project Limits From Interstate Highway 35 (I-35) to
TITLE VI COMPLAINT FORM
 [CITY SEAL/EMBLEM] The Capital City of the Palm Beaches TITLE VI COMPLAINT FORM Title VI of the 1964 Civil Rights Act requires that "No person in the United States shall, on the ground of race, color or
[CITY SEAL/EMBLEM] The Capital City of the Palm Beaches TITLE VI COMPLAINT FORM Title VI of the 1964 Civil Rights Act requires that "No person in the United States shall, on the ground of race, color or
FAMILY INDEPENDENCE ADMINISTRATION Seth W. Diamond, Executive Deputy Commissioner
 FAMILY INDEPENDENCE ADMINISTRATION Seth W. Diamond, Executive Deputy Commissioner James K. Whelan, Deputy Commissioner Policy, Procedures and Training Lisa C. Fitzpatrick, Assistant Deputy Commissioner
FAMILY INDEPENDENCE ADMINISTRATION Seth W. Diamond, Executive Deputy Commissioner James K. Whelan, Deputy Commissioner Policy, Procedures and Training Lisa C. Fitzpatrick, Assistant Deputy Commissioner
Tax News Mexico April 2017
 April 2017 Payroll Tax Receipt Complemento V.1.2 Payroll Tax Receipt (Complemento V.1.2) The Complemento has been in force since January 1, 2017. SAT gave an extension until March 31, 2017 to comply with
April 2017 Payroll Tax Receipt Complemento V.1.2 Payroll Tax Receipt (Complemento V.1.2) The Complemento has been in force since January 1, 2017. SAT gave an extension until March 31, 2017 to comply with
Formulario de Postulación Universidad Católica Santo Toribio De Mogrovejo Estudiante de Intercambio Application Form / Exchange Student
 Formulario de Postulación Universidad Católica Santo Toribio De Mogrovejo Estudiante de Intercambio Application Form / Exchange Student Información Personal Personal Information: Nombre FIrst Name Apellido
Formulario de Postulación Universidad Católica Santo Toribio De Mogrovejo Estudiante de Intercambio Application Form / Exchange Student Información Personal Personal Information: Nombre FIrst Name Apellido
Notice of Alleged Safety or Health Hazards Aviso de Presuntos Peligros de Seguridad o de Salud. Kentucky Labor Cabinet Gabinete de Trabajo de Kentucky
 Notice of Alleged Safety or Health Hazards Aviso de Presuntos Peligros de Seguridad o de Salud Gabinete de Trabajo de Kentucky Departamento de Normas de Trabajo Division of Occupational Safety and Health
Notice of Alleged Safety or Health Hazards Aviso de Presuntos Peligros de Seguridad o de Salud Gabinete de Trabajo de Kentucky Departamento de Normas de Trabajo Division of Occupational Safety and Health
AGENCY POLICY: REVIEW OF NOTICE OF PRIVACY PRACTICES
 AGENCY POLICY: REVIEW OF NOTICE OF PRIVACY PRACTICES SCOPE OF POLICY This policy applies to all agency staff members. Agency staff members include all employees, trainees, volunteers, consultants, students,
AGENCY POLICY: REVIEW OF NOTICE OF PRIVACY PRACTICES SCOPE OF POLICY This policy applies to all agency staff members. Agency staff members include all employees, trainees, volunteers, consultants, students,
Requesting Accommodations SAT and ACT. Sign and return the Parent permission form to the SSD Coordinator
 Requesting Accommodations SAT and ACT SAT Sign and return the Parent permission form to the SSD Coordinator SSD Coordinator submits information online to College Board The deadline for accommodations approval
Requesting Accommodations SAT and ACT SAT Sign and return the Parent permission form to the SSD Coordinator SSD Coordinator submits information online to College Board The deadline for accommodations approval
Medicaid Renewals. Create Account
 Medicaid Renewals In order to have your Medicaid eligibility reassessed through the Maryland Health Connection, create an account and submit a new application. NOTE: YOU MUST COMPLETE THE SPECIAL ENROLLMENT
Medicaid Renewals In order to have your Medicaid eligibility reassessed through the Maryland Health Connection, create an account and submit a new application. NOTE: YOU MUST COMPLETE THE SPECIAL ENROLLMENT
SPANISH RESIDENCE VISA/AUTHORISATION FOR THE PURCHASE OF PROPERTY OF 500,000 EUROS
 SPANISH RESIDENCE VISA/AUTHORISATION FOR THE PURCHASE OF PROPERTY OF 500,000 EUROS LEGAL FRAMEWORK Law 14/2013 of 27th September aims to support entrepreneurs with their international expansion and to
SPANISH RESIDENCE VISA/AUTHORISATION FOR THE PURCHASE OF PROPERTY OF 500,000 EUROS LEGAL FRAMEWORK Law 14/2013 of 27th September aims to support entrepreneurs with their international expansion and to
EL CENTRO REGIONAL MEDICAL CENTER FINANCIAL ASSISTANCE APPLICATION INSTRUCTIONS
 EL CENTRO REGIONAL MEDICAL CENTER FINANCIAL ASSISTANCE APPLICATION INSTRUCTIONS Instructions As part of our commitment to serve the community, El Centro Regional Medical Center elects to provide financial
EL CENTRO REGIONAL MEDICAL CENTER FINANCIAL ASSISTANCE APPLICATION INSTRUCTIONS Instructions As part of our commitment to serve the community, El Centro Regional Medical Center elects to provide financial
Job Title: USTT - VIRGINIA OFFICE. Status History Status Change Date Changed By Make Offer 11/02/2018 Rodriguez, Christina New Application 11/02/2018
 Applicant: hernandez, suzette Job Title: USTT - VIRGINIA OFFICE Application Job Title: USTT - VIRGINIA OFFICE Source: Career center Recruiter: Christina Rodriguez Date Applied: 11/02/2018 Hiring Manager:
Applicant: hernandez, suzette Job Title: USTT - VIRGINIA OFFICE Application Job Title: USTT - VIRGINIA OFFICE Source: Career center Recruiter: Christina Rodriguez Date Applied: 11/02/2018 Hiring Manager:
INSTRUCTIONS FOR FILLING OUT FINANCIAL AFFIDAVIT FOR CHILD SUPPORT INSTRUCCIONES PARA COMPLETAR EL AFIDÁVIT DE FINANZAS PARA MANUTENCIÓN DE MENORES
 INSTRUCTIONS FOR FILLING OUT FINANCIAL AFFIDAVIT FOR CHILD SUPPORT INSTRUCCIONES PARA COMPLETAR EL AFIDÁVIT DE FINANZAS PARA MANUTENCIÓN DE MENORES THIS FORM MUST BE SIGNED BEFORE A NOTARY PUBLIC. ESTE
INSTRUCTIONS FOR FILLING OUT FINANCIAL AFFIDAVIT FOR CHILD SUPPORT INSTRUCCIONES PARA COMPLETAR EL AFIDÁVIT DE FINANZAS PARA MANUTENCIÓN DE MENORES THIS FORM MUST BE SIGNED BEFORE A NOTARY PUBLIC. ESTE
Lump Sum Final Check Contribution to Deferred Compensation
 Memo To: ERF Members The Employees Retirement Fund has been asked by Deferred Compensation to provide everyone that has signed up to retire with the attached information. Please read the information from
Memo To: ERF Members The Employees Retirement Fund has been asked by Deferred Compensation to provide everyone that has signed up to retire with the attached information. Please read the information from
TITLE VI & RELATED PROGRAMS DISCRIMINATION COMPLAINT FORM
 TITLE VI & RELATED PROGRAMS DISCRIMINATION COMPLAINT FORM How can I file a discrimination complaint? If you believe a United States Department of Transportation (USDOT) recipient has discriminated against
TITLE VI & RELATED PROGRAMS DISCRIMINATION COMPLAINT FORM How can I file a discrimination complaint? If you believe a United States Department of Transportation (USDOT) recipient has discriminated against
Salaried/Exempt Time Reporting
 Salaried/Exempt Time Reporting GOAL: Exempt Employees able to report: 1.Benefits Time 2.Positive Time Objetivo: Los empleados que NO reciben un sueldo por hora, pueden reportar lo siguiente: 1.Tiempo en
Salaried/Exempt Time Reporting GOAL: Exempt Employees able to report: 1.Benefits Time 2.Positive Time Objetivo: Los empleados que NO reciben un sueldo por hora, pueden reportar lo siguiente: 1.Tiempo en
Circuit Court for TRIBUNAL DE CIRCUITO DE
 Circuit Court for TRIBUNAL DE CIRCUITO DE City or County (Ciudad o Condado) Case No. Name (Nombre) vs. (contra) Name (Nombre) Street Address (Dirección) Apt. # Street Address (Dirección) Apt. # City Ciudad
Circuit Court for TRIBUNAL DE CIRCUITO DE City or County (Ciudad o Condado) Case No. Name (Nombre) vs. (contra) Name (Nombre) Street Address (Dirección) Apt. # Street Address (Dirección) Apt. # City Ciudad