SITUACIÓN ACTUAL DE LA INMUNOTERAPIA EN EL MELANOMA METASTÁTICO CASO(S) CLÍNICO(S) Y ACTUALIZACIÓN
|
|
|
- Clara Padilla Cáceres
- hace 6 años
- Vistas:
Transcripción
1 SITUACIÓN ACTUAL DE LA INMUNOTERAPIA EN EL MELANOMA METASTÁTICO CASO(S) CLÍNICO(S) Y ACTUALIZACIÓN Mª Carmen Alonso López Servicio de Oncología Médica. Hospital de Albacete

2 20 ENERO 2017
3 1º Caso clinico: paciente que va bien con inmunoterapia 71 Añós. No alergias medicamentosas. No DM. No HTA. Dislipemia (Atorvastatina). FEBRERO/2006: ADENOCA PRÓSTATA (pt2a). Prostatectomía radical laparoscópica. Revisiones en Urología, sin recaida. JULIO/2011: MELANOMA EN PIEL DE REGION DORSAL (Seguía revisiones por múltiples nevus (más de 100) sobre todo en tronco) 1º EXÉRESIS SIMPLE (25/07/11): melanoma, Breslow 2,5 mm. Clark III. Con ulceración, + TC Sin enfermedad a distancia. -- AMPLIACIÓN DE MÁRGENES (-) Y BSGC (29/08/11): CENTINELA AXILAR IZQ: MICROMTS DE MELANOMA. 3º) LINFADENECTOMÍA AXILAR IZQ (26/09/11): (0/15) Se desestimó adyuvancia con IFN a dosis altas por edad. (Seguimiento en Derma y C.Plástica)
4 Caso clinico (2) A los 3.5 años : DESDE ENERO/2014: MULTIPLES METÁSTASIS EN TRÁNSITO RESECADAS EN REGION PERIESCAPULAR: FEB- 2014: uno de 2cm y otro satélite de 5mm. (TAC entonces SIN ENF A DISTANCIA) OCT Y NOV/2014: 2 EXÉRESIS DE MÁS MTX EN TRÁNSITO. DIC 2014 Y ENERO-2015: Nueva CIRUGIA DE CUTÁNIDES, + COBERTURA CON AUTOINJERTO DE MUSLO. OCT Nueva exéresis de metastasis en tránsito en la zona (+ TAC OCT-215 SIN ENF A DISTANCIA) ENERO-2016: NUEVA CIRUGIA DE MTS CUTANEAS: (6 nódulos de metástasis de melanoma, cuatro subcutáneos y dos en dermis profunda que no alcanza los bordes de resección ( un nódulo subcutáneo a menos de 1 mm del borde quirúrgico medial ).

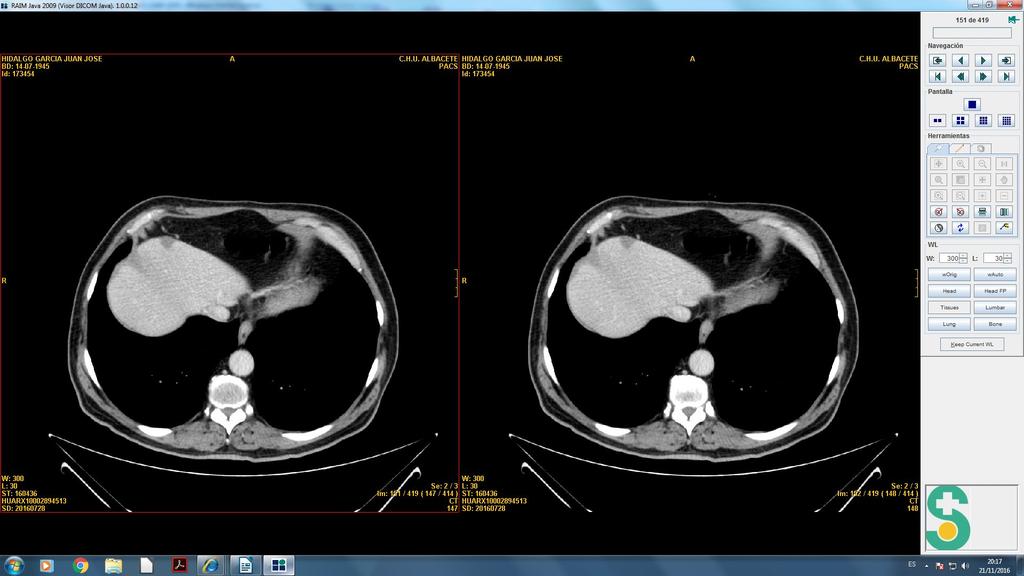
5 Caso clinico (3) ABRIL-2016: SE REMITE A ONCOLOGIA POR PROGRESION PULMONAR - TAC (ABRIL-2016) -Milimetricos nódulos pulmonares bilaterales de nueva aparición. Los mayores el Apical dcho de 8 mm) Apical iz de 6 mm), Basal anterior inferior LSD, Basal medial inferior LIIz
6 Caso clínico (4) PACIENTE ECOG 0, LDH NORMAL Y ENFERMEDAD ESCASA: CANDIDATO PARA INMUNOTERAPIA SE SOLICITA AUTORIZACION PARA TRATAMIENTO CON PEMBROLIZUMAB: que COMIENZA EN MAYO RECIBIDO POSTERIORMENTE B-RAF MUTADO --- Tras 4º:TAC (28-JULIO-2016): - RESPUESTA PULMONAR nódulos HAN DISMINUIDO DE TAMAÑO. - Pero APARICION DE VARIAS LESIONES FOCALES SOLIDAS ESPLENICAS compatibles con metastasis (En hígado hay varias lesiones hipodensas informados como quistes simples) PERO ESTE TAC CON MEJOR DEFINICION, LA LESION DEL SGM IV DE 16 mm SE ETIQUETA COMO METASTASIS

7
8 Caso Clínico (5) qué hacer? TAC DE DISTINTA DEFINICION, EXISTE RESPUESTA DE LOS NODULOS PULMONARES + LDH NORMAL + PACIENTE ASINTOMATICO. ANTE POSIBILIDAD DE PSEUDO-PROGRESION, SE DECIDE CONTINUAR TTO X 3 MESES (julio a octubre- 2016) EN TAC OCTUBRE-2016 HAY RESPUESTA COMPLETA DE LAS MTS PULMONARES PERO
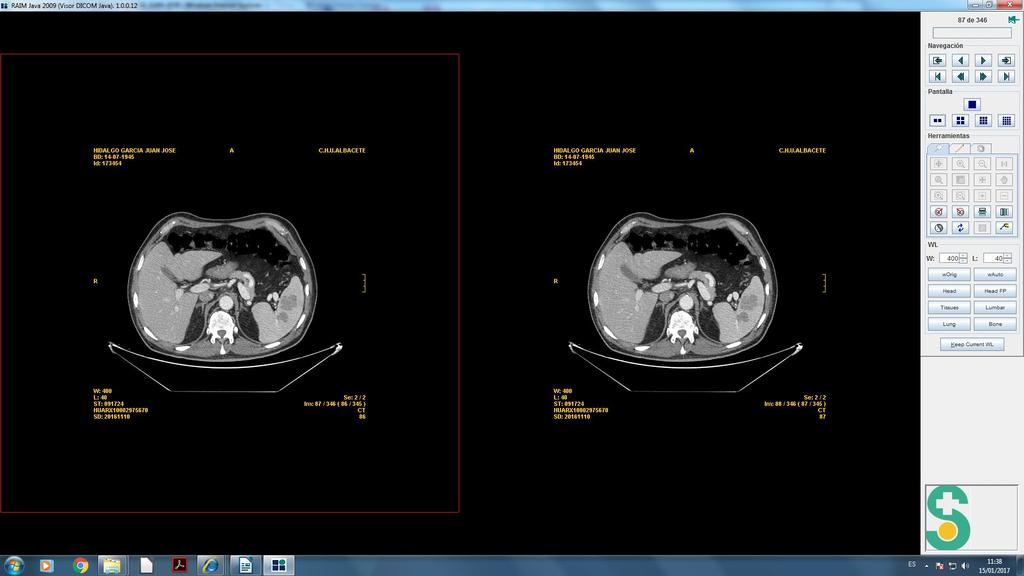
9 Caso clinico (6) ACUDE A URGENCIAS EL 31-10, POR DOLOR ABDOMINAL + DIARREA ABUNDANTE Y FIEBRE DE 39ºc CON SINCOPE (EL 112 REGISTRA HIPOTENSION MARCADA) TAC (OCT-2016) DESAPARICION DE LOS NODULOS PULMONARES PREVIOS PERO Aparición de MASA HIPODENSA-implante de centro de aspecto necrótico, de 7x7 cm. en FII y que contacta con asas de delgado condicionado discreta dilatación segmentaria por probable suboclusión intestinal. + Aumento de las lesiones focales sólidas esplénicas (la mayor de 32 mm ) + En hígado persisten los quistes simples mm y la lesión sólida periférica en segmento 4 de 16 mm. Mínimo aumento (?) De lesión lítica inespecífica del hueso ilíaco de 8 mm. aprox. (antes 6,5 mm).
10
11 Caso clinico (7) Resolución Valorado en Comité, Se sugiere: PCR elevada en paciente con inmunoterapia, no se puede descartar por la imagen eventual microperforacion con abcesificación, persistiendo dolor abdominal a pesar de corticoides y antibióticos, y se decide CIRUGIA LAPAROTOMIA : halla implante peritoneal infiltrando un asa de i.delgado, que se reseca. AP. METASTASIS DE MELANOMA ACTUALMENTE: Pendiente de recuperacion de complicaciones post-cirugia (precisó 2 cirugias x peritonitis x dehiscencia) con TAC mostrando multiples imágenes de abcesos abdominales PREVISTO INICIAR TTO CON DOBLE BLOQUEO ANTI BRAF-ANTI MEK
12
13

14 Tumor Immunology: Overview 3 Tumor Perforin granzyme Cytokines (IL-2) Resting T cell Activated T cell 2 T-cell clonal expansion Tumor antigen TCR 1 MHC B7 Dendritic cell CD28 Lymph node
15 PUNTOS DE CONTROL PARA LA INMUNOTERAPIA ganglio tumor
 Approved 2011 2013 at first line")
16 IPILIMUMAB El pionero Ab anti Cytotoxic T-Lymphocyte Associated Ag-4 (CTLA-4) Approved at first line at Europe
17 Ipilimumab, gp100, or Both: OS in Advanced Melanoma Median OS, Mos Ipilimumab + gp100 (n = 403) 10.0 Ipilimumab alone (n = 137) 10.1 gp100 alone (n = 136) OS (%) 80 HR P Value < ORR: 10.9% 60 2-yr OS, % Ipi + gp100 22% Ipi alone: 24% Gp100 alone: 14% Yrs % OS, Hodi FS, et al. N Engl J Med. 2010;363: Yr 1 Ipi + gp100 4 Ipi + Placebo gp100 + Placebo
18 Phase II and Phase III Trials of Ipilimumab: OS Plateau at Yr 3 Proportion Alive 1.0 Median OS: 11.4 mos (95% CI: ) yr OS rate: 22% (95% CI: 20% to 24%) Ipilimumab Censored 0 0 Pts at Risk, n Ipilimumab Mos Schadendorf D, et al. J Clin Oncol. 2015;33: Slide credit: clinicaloptions.com
19
20 OS: 11.2 vs 9.1 PFS: 2.7 m
21
22 Que nos enseñó el Ipilimumab? Respuesta escasas (11-15%) MEJOR SI Biología Tumoral Favorable Bajo volumen tumoral, Normal LDH, Peor visceral % control de la enfermedad muy prolongado SOLO CON 4 DOSIS (12 Semanas) ( PRECIO ) PRECISA TIEMPO (3 O MAS MESES) PARA VER RESPUESTA (no es buena opción si se requiere respuesta rápida) PATRON DE RESPUESTA INHABITUAL. Pseudoprogresion inicial antes de respuesta posterior (hasta 25% casos). Esperar PROBLEMATICA TOXICIDAD INMUNOMEDIADA: EFECTOS ADVERSOS RELACIONADOS CON SU MECANISMO DE ACCION Centros con experiencia por la toxicidad Y colaboración del paciente
23 Summary of CTLA-4 Blockade Immune-Mediated Toxicities Toxicity of ipilimumab appears to be dose related Common (> 20%) Rash, GI: Episcleritis/uveitis pruritus Fevers, chills, lethargy Diarrhea/colitis Occasional (3% to 20%) Hepatitis/liver enzyme abnormalities Endocrinopathies: hypophysitis, thyroiditis, adrenal insufficiency Vitiligo Rare (< 2%) Pancreatitis Nephritis Neuropathies, Guillain-Barré, myasthenia gravis Lymphadenopathy (sarcoid) Thrombocytopenia Toxic epidermal necrolysis, Stevens-Johnson syndrome IrAEs occurred in about 64.2% of patients treated with ipilimumab in several phase IWeber -III studies of grade 3 andweber 4 events) JS, et al.(with J Clin20-30% Oncol. 2012;30: JS, et al. J Clin Oncol. 2015;[Epub ahead of print].

24
25 PUNTOS DE CONTROL PARA LA INMUNOTERAPIA Ganglio Tumor

 for unresectable or metastatic")
26 PD-1 Inhibitors: Melanoma 2015 Nivolumab + Single agent (3 mg/kg q2w) for unresectable or metastatic melanoma with or without a BRAF V600 mutation **** Flat dose 240 mg c/2w ***** + In combination with ipilimumab for unresectable or metastatic melanoma Nivolumab 1 mg/kg + ipilimumab 3 mg/kg q3w x 4 then nivolumab 3 mg/kg q2w Pembrolizumab + Single agent (2 mg/kg q3w) for unresectable or metastatic melanoma
27 Estudios anti PD1 POST-IPI (PACIENTE IPI-REFRACTARIOS) NIVOLUMAB vs Chemotherapy; Checkmate-037 PEMBROLIZUMAB vs Chemotherapy; KEYNOTE-002: **** PRIMERA LINEA VS QUIMIOTERAPY; NIVOLUMAB vs Chemotherapy CheckMate 066: VS IPILIMUMAB PEMBRO vs Ipilimumab KEYNOTE-006: NIVO + IPI vs NIVO vs IPI Checkmate-067:
28 ANTI PD1: Nivolumab Pembrolizumab in Ipilimumab-Refractory Pts Comparison Pts, n (IPI-R) FDA-approved schedule ORR, % (95% CI) Grades 3/4 drug-related toxicities, % * 2º LINEA Nivolumab (Checkmate-037) Pembrolizumab (KEYNOTE-002) (2 doses) 120 (preliminary subset) mg/kg IV every 2 wks 2 mg/kg IV every 3 wks 32 (24-41) 5 21 (15-28) 8
29 Phase III Checkmate-037: Nivolumab vs Chemotherapy in Ipilimumab-Refractory Pts Stratified by PD-L1 expression (+ vs - or indeterminate)*, BRAF wild type vs V600 mutant, best overall response prior to anti CTLA-4 (clinical benefit vs no clinical benefit) Pts with advanced melanoma who progressed on or after ipilimumab (and BRAF, if BRAF V600+) Nivolumab 3 mg/kg IV q2w (n = 268) Open Label Investigator s choice of chemotherapy: Dacarbazine 1000 mg/m2 q3w or Carboplatin AUC 6 IV + Paclitaxel 175 mg/m2 q3w (n = 102) Treat until Progression OR Unacceptable toxicity Pts receiving nivolumab may be treated beyond initial progression if considered by the investigator to be experiencing clinical benefit and tolerating study drug *Positive: 5% tumor cell surface staining cutoff by IHC. Weber JS, et al. Lancet Oncol. 2015;16: Slide credit: clinicaloptions.com
30 Nivolumab vs Chemotherapy in Ipilimumab-Refractory Pts: ORR and Safety Treatment N CR + PR, n ORR*, % (95% CI) CR PR SD PD UNK Best Overall Response,* % Central review Nivolumab (4 CR) 32 (24-41) ICC 47 5 (0 CR) 11 (4-23) *Confirmed response. Independent radiology review committee based on RECIST 1.1. Grade 3/4 toxicity incidence higher with chemotherapy (32%) vs nivolumab (9%) Most frequent adverse events of any grade ( 10%) Nivolumab: fatigue, pruritus, and diarrhea Chemotherapy: fatigue, nausea, vomiting, anemia, reduced appetite, diarrhea, constipation, arthralgia, and alopecia Weber JS, et al. Lancet Oncol. 2015;16: Slide credit: clinicaloptions.com
31 KEYNOTE-002: Pembrolizumab vs Chemotherapy in Ipi-Refractory Melanoma Stratified by ECOG PS (0 vs 1); LDH (normal vs 110% ULN); BRAF status (wild type vs V600 mutant) PHASE II: Pts with advanced melanoma who progressed on or after Ipi (and targeted therapy, if BRAF V600+) (N = 540) Pembrolizumab 2 mg/kg IV q3w (n = 180) Pembrolizumab 10 mg/kg IV q3w (n = 181) Investigators choice of chemotherapy* (n = 179) *Carboplatin + paclitaxel, paclitaxel alone, carboplatin alone, dacarbazine, or temozolomide. Pts with PD confirmed by independent central review could cross over to pembrolizumab treatment after the first 3-mo assessment. Primary endpoint: PFS, OS Ribas A, et al. Lancet Oncol. 2015;16: Secondary endpoints: ORR, DoR Slide credit: clinicaloptions.com
32 KEYNOTE-002: Efficacy and Safety ORR, % PFS (%) An international, randomized phase II study in pts with advanced melanoma with PD within 24 wks after 2 Ipi doses 60 Grade 3/4 toxicity incidence higher with chemotherapy (26%) vs pembrolizumab (11% at 2 mg/kg and 14% at 10 mg/kg) Most frequent adverse events of any grade ( 10%) Pembro 2 mg/kg q3w 21 Pembro 10 mg/kg q3w 25 Chemotherapy 4 Pembrolizumab: fatigue, pruritus, and rash Chemotherapy associated primarily with grade 1/2 fatigue, nausea, vomiting, anemia, reduced appetite, alopecia Mos Ribas A, et al. Lancet Oncol. 2015;16: Slide credit: clinicaloptions.com
33 KEYNOTE-002: Efficacy and Safety NOT dose response relationship (Pembro at 2 mg/kg or 10 mg/kg did not affect outcomes) 100 PFS (%) 80 Results updated al European Society for Medical Oncology (ESMO) 2016 ORR, % PFS 2 years % OS m 24 m OS % Pembro 2 mg/kg q3w Pembro 10 mg/kg q3w Chemotherapy 4 <1 11 * 30 * Mos Ribas A, et al. Lancet Oncol. 2015;16: Slide credit: clinicaloptions.com
34 Estudios anti PD1 POST-IPI (PACIENTE IPI-REFRACTARIOS) NIVOLUMAB vs Chemotherapy; Checkmate-037 PEMBROLIZUMAB vs Chemotherapy; KEYNOTE-002: **** PRIMERA LINEA VS QUIMIOTERAPY; NIVOLUMAB vs Chemotherapy CheckMate 066: VS IPILIMUMAB PEMBRO vs Ipilimumab KEYNOTE-006: NIVO + IPI vs NIVO vs IPI Checkmate-067:
35 Phase III CheckMate 066: First-line Nivolumab vs Chemotherapy Stratified by PD-L1 status, M-stage Unresectable, treatment-naive stage III or IV melanoma; BRAF wild type; ECOG PS 0-1; 18 yrs of age or older (N = 418) Nivolumab 3 mg/kg IV q2w + Placebo IV q3w (n = 210; 206 treated) Placebo IV q2w + Dacarbazine 1000 mg/m2 IV q3w (n = 208; 205 treated) Treat until progression* or unacceptable toxicity * Pts may be treated beyond initial RECIST v1.1 defined progression if considered by the investigator to be experiencing clinical benefit and tolerating study drug. Primary endpoint: OS Secondary endpoints: PFS, ORR, PD-L1 correlates Robert C, et al. N Engl J Med. 2015;372: Slide credit: clinicaloptions.com
36 First-line Nivolumab vs Chemotherapy: OS Objective RR: 40.0% with nivolumab vs 13.9% with chemo (P <.001) (respuesta en dias pocas semanas) Significantly better OS with nivolumab vs dacarbazine 100 HR 0.42 (99.79% CI: ; P <.001) 1-yr OS: 73% Pts Surviving (%) yr OS: 42% 40 Median OS, Mos (95% CI) 20 Nivolumab Dacarbazine NR 10.8 ( ) Robert C, et al. N Engl J Med. 2015;372: M os Slide credit: clinicaloptions.com
37 First-line Nivo vs Chemotherapy: PFS Pts Without Progression (%) 100 Nivolumab Dacarbazine 80 6-mo PFS: 48% 60 Median PFS, Mos (95% CI) 5.1 ( ) 2.2 ( ) HR: 0.43 (95% CI: ; P <.001) Nivolumab (n = 210) 40 6-mo PFS: 19% 20 Dacarbazine (n = 208) M os 0 Robert C, et al. N Engl J Med. 2015;372: Slide credit: clinicaloptions.com
38
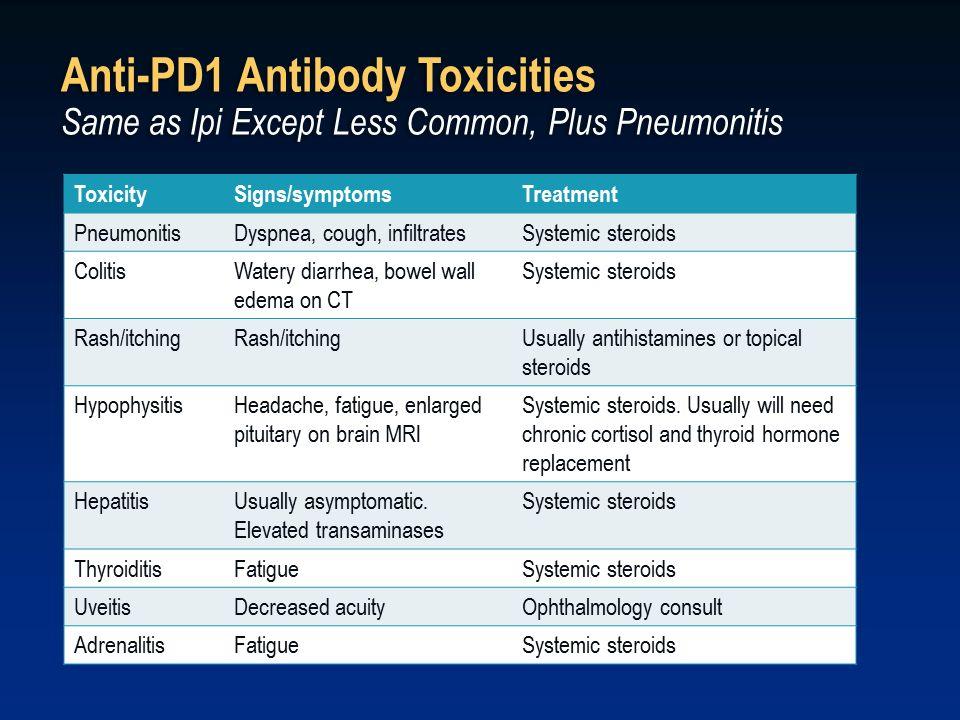
39 PD-1/PD-L1 Blockade Immune-Mediated Toxicities Occasional (5% to 20%) Fatigue Rash: maculopapular and pruritus Topical treatments Diarrhea/colitis Initiate steroids early, taper Infusion reactions Endocrinopathies: thyroid, adrenal, hypophysitis Infrequent (< 5%) Pneumonitis Grade 3/4 toxicities uncommon slowly Hepatitis/liver enzyme abnormalities Topalian SL, et al. N Engl J Med. 2012;366: Patnaik A, et al. ASCO Abstract Brahmer JR, et al. N Engl J Med. 2012;366: Herbst RS, et al. ASCO Abstract 3000.
40
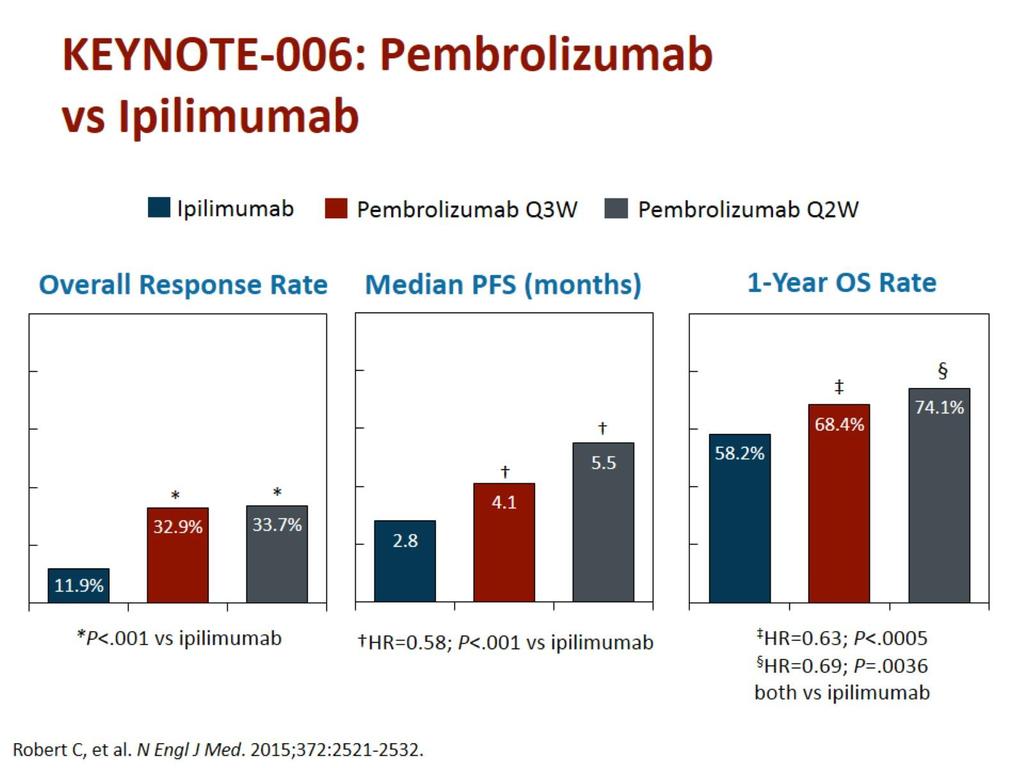
41 KEYNOTE-006: Pembrolizumab (2 Doses) vs Ipilimumab in Stage III/IV Melanoma A multicenter, randomized, phase III study (1º linea immuno) Stratified by ECOG PS (0 vs 1), line of therapy (first vs second), PD-L1 status (positive vs negative) Pembrolizumab 10 mg IV q2w for up to 2 yrs Unresectable stage III or IV melanoma; 1 prior therapy, excluding checkpoint inhibitors; ECOG PS 0-1; 18 yrs of age or older (N = 834) Pembrolizumab 10 mg IV q3w for up to 2 yrs Ipilimumab 3 mg/kg IV once q3w for 4 doses Primary endpoint: PFS, OS Secondary endpoint: ORR, DoR, safety Robert C, et al. N Engl J Med. 2015;372: Slide credit: clinicaloptions.com
42 KEYNOTE-006: Survival Efficacy at First Interim Analysis of Pembro vs Ipi PFS OS (%) Mos OS PFS (%) Mos HR (95% CI) P Value Median OS (95% CI), Mos Rate at 12 Mos, % Treatment Arm Median PFS Rate at (95% CI), 6 Mos, % Mos Pembro q2w 5.5 ( ) ( ) < NR (NR-NR) ( ) Pembro q3w 4.1 ( ) ( ) < NR (NR-NR) ( ).0036 Ipi 2.8 ( ) 26.5 NR (12.7-NR) 58.2 Robert C, et al. N Engl J Med. 2015;372: RESPUESTA EN LA PG SIGUIENTE. HR (95% CI) P Value Slide credit: clinicaloptions.com
43
44
45 Checkmate-067: Nivo + Ipi vs Nivo vs Ipi for First-line A randomized, double-blind phase III study Stratified by tumor PD-L1 status (positive vs negative/indeterminate), BRAF mutation status (V600 mutation positive vs wild type), and AJCC metastasis stage (M0, M1a, or M1b vs M1c) Unresectable, treatment-naive stage III or IV melanoma; ECOG PS 0-1; 18 yrs of age or older (N = 945) Nivo 1 mg/kg IV + Ipi 3 mg/kg IV every 3 wks for 4 doses Nivo 3 mg/kg IV every 2 wks until PD or unacceptable AE Placebo + Nivo 3 mg/kg IV every 2 wks for 4 doses Nivo 3 mg/kg IV every 2 wks until PD or unacceptable AE Placebo + Ipi 3 mg/kg IV every 3 wks for 4 doses Placebo IV every 2 wks until PD or unacceptable AE Primary endpoint: OS, PFS Secondary endpoint: ORR, OS by PD-L1, safety DOSIS IPI Y NIVO? Larkin J, et al. N Engl J Med. 2015;373:23-34.
46
47 Proportion Alive and Progression Free CheckMate 067: Improved PFS With Nivo + Ipi or Nivo Alone vs Ipi Alone Nivo + Ipi (n = 314) Nivo (n = 316) Ipi (n = 315) 11.5 ( ) 6.9 ( ) 2.9 ( ) HR (99.5% CI) vs Ipi 0.42 ( )* 0.57 ( )* _ HR (95% CI) vs Nivo 0.74 ( ) Median PFS, mos (95% CI) Nivo + Ipi Nivo Ipi *Stratified log-rank P < vs Ipi Mos Exploratory endpoint. Study not powered to detect a statistical difference between Nivo + Ipi and Nivo. 21
48
49 CheckMate 067: Nivo + Ipi Provides Most Benefit for PD-L1lo, Similar to Nivo for PD-L1hi PD-L1 5%* Median PFS, Mos HR Nivo + Ipi Nivo alone Ipi alone Mos Median PFS, Mos HR 0.42 Nivo + Ipi Nivo alone Ipi alone 100 PFS (%) 80 PFS (%) PD-L1 < 5%* Mos *Per validated PD-L1 IHC assay based on PD-L1 staining of tumor cells in a section of at least 100 evaluable tumor cells. Larkin J, et al. N Engl J Med. 2015;373: Slide credit: clinicaloptions.com
50 CheckMate 067: Treatment-Related AEs Associated With Nivo and Ipi Select Treatment-Related AEs, % Nivo + Ipi (n = 313) Nivo (n = 313) Ipi (n = 311) All Grades Grade 3/4 All Grades Grade 3/4 All Grades Grade 3/4 Any select AE Skin Pruritus Rash Maculopapular rash <1 < <1 2 <1 Gastrointestinal Diarrhea Colitis < Hepatic ALT increase AST increase <1 Endocrine Hypothyroidism < < Pulmonary Pneumonitis <1 <1 2 2 <1 <1
51
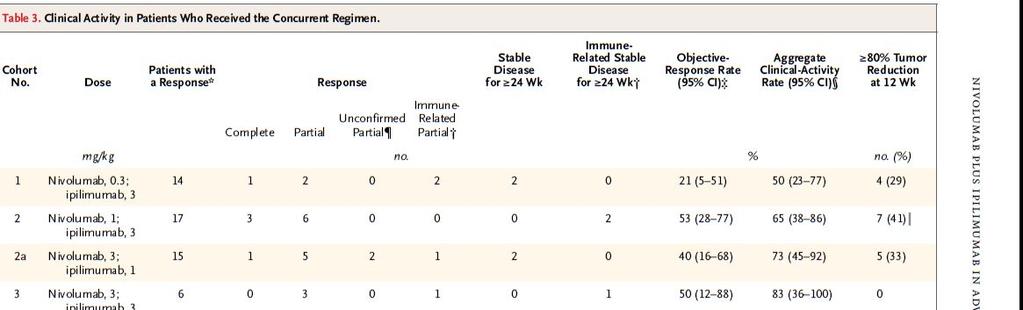
52 Ipilimumab plus pembrolizumab?? ASCO 2016 A Non-randomized expansion cohort combining pembrolizumab pembrolizumab (2 mg/kg every three weeks) + ipilimumab (1 mg/kg for four doses) Median follow-up of 10 months, the ORR 57 % (including 10 % RC and 47 % PR). PFS was 70 % at 6 months. Grade 3 or 4 toxicity was observed in 42 % of patients; immune-related adverse events were seen in 58 % of patients, and 25 % experienced grade 3 or 4 immune-related toxicity. Only 25 % of patients needed to stop therapy due to toxicity.

53 MULTIPLES PREGUNTAS Y DUDAS
54
55 Desmontar lo que sabíamos con el Ipi?? IPILIMUMAB Respuesta (11-15%), 25-30% prolongado RESPUESTA PRECISA TIEMPO (3 O MAS MESES) PATRON DE RESPUESTA INHABITUAL. SOLO CON 4 DOSIS (12 Semanas) - Precio* TOXICIDAD SERIA INMUNOMEDIADA: NIVO PEMBROLIZUMAB RESPUESTAS > 40% (TB VISCERAL) RESPUESTA RAPIDA ( B-RAF?) Prolongadas? Poco tiempo
56 ANTI-PD1 OR ANTI-BRAFi? No Association Between BRAF or NRAS Mutation and Response to Ipilimumab BRAF-i Followed by Ipilimumab or Ipilimumab Followed by a BRAFi: OS: better for ipi in first line BRAF inhibitor, ipilimumab: 9.9 mos (95% CI: ) Ipilimumab, BRAF inhibitor: 14.5 m (95% CI: ) Median OS in patient subgroups (ipi-brafi vs BRAFi-ipi) Elevated LDH: 14 (95% CI: ) vs 7.5 mos (95% CI: ) Brain metastasis: 12.3 (95% CI: ) vs 7.5 mos (95% CI: ) NO DATOS CON ANTI-PD1 (los datos del pembro que eran mejor en B-RAF MUTADOS ANTES DE TERAPIA ANTI-BRAF)
57 Phase III Dabrafenib/Trametinib Nivo/Ipi vs Nivo/Ipi Dabrafenib/Trametinib Sequencing study combining immunotherapy and BRAF/MEK Progression inhibition in stage III/IV melanoma Unresectable, treatment-naive stage III or IV melanoma; ECOG PS 0-1; BRAF V600E/K mutation (Planned N = 300) Dabrafenib 150 mg PO BID + Trametinib 2 mg PO QD Nivo 1 mg/kg + Ipi 3 mg/kg q3w for 4 doses, then Nivo 3 mg/kg q2w Nivo 1 mg/kg + Ipi 3 mg/kg q3w for 4 doses, then Nivo 3 mg/kg q2w Dabrafenib 150 mg PO BID + Trametinib 2 mg PO QD Primary endpoint: 2-yr OS rate Secondary endpoints: PFS, ORR, safety ClinicalTrials.gov. NCT Slide credit: clinicaloptions.com
58
59 Desmontar lo que sabíamos con el Ipi?? IPILIMUMAB Respuesta (11-15%), 25-30% prolongado RESPUESTA PRECISA TIEMPO (3 O MAS MESES) PATRON DE RESPUESTA INHABITUAL. SOLO CON 4 DOSIS (12 Semanas) - Precio* TOXICIDAD SERIA INMUNOMEDIADA: NIVO PEMBROLIZUMAB RESPUESTAS > 40% (TB VISCERAL) RESPUESTA RAPIDA ( B-RAF?) Prolongadas? Poco tiempo PRACTICAMENTE NO PSEUDO-PROGRESION TTO HASTA PROGRESION?? Precio+++
60 Hay Pseudoprogresión (patrón atipico de respuesta?) con antipd1? Immune-related response criteria have been proposed with ipilimumab and potentially other immunotherapies. Of 655 patients with pembrolizumab; who survived at least 12 weeks, ONLY 14 % had progressive disease by RECIST but not by immune-related response criteria (And OS 2-year was 37.5%, vs 17.3 % in those with progressive disease based upon both criteria). BUT Among the 327, pseudoprogression ( 25 percent increase in tumor burden NOT confirmed at repeat imaging) was observed ONLY in 24 cases (7%), of which 15 occurred by 12 weeks of imaging, and nine were later. (93% WERE AUTHENTIC PROGRESSION )
61 Expert opinion: In a patient who has minor to moderate increase in disease burden by imaging, but who is otherwise feeling well, with no evidence of decline, continuing treatment with the same immunotherapy is reasonable until the time of a confirmatory scan. However, it is important to emphasize that this is a relatively uncommon phenomenon, and patients who are experiencing increasing cancer-related symptoms or clinical decline should not be continued on the same treatment. OTRA COSA ES QUE TENGAMOS ALGO MEJOR QUE OFRECERLES
62 Tratamiento hasta progresión?? Para qué? Si se retira van igual? A retrospective, unpowered analysis suggested that these patients still did at least as well as those patients who received the full treatment Entonces xq no quitarlo antes? Cuando?
63
64 Desmontar lo que sabíamos con el Ipi?? IPILIMUMAB Respuesta (11-15%), 25-30% prolongado NIVO PEMBROLIZUMAB RESPUESTAS > 40% (TB VISCERAL) RESPUESTA RAPIDA ( B-RAF?) Prolongadas? Poco tiempo RESPUESTA PRECISA TIEMPO (3 O MAS MESES) PATRON DE RESPUESTA INHABITUAL. PRACTICAMENTE NO PSEUDO-PROGRESION TTO HASTA PROGRESION?? Precio+++ SOLO CON 4 DOSIS (12 Semanas) Precio* MUCHO MENOS TOXICO (PERO NO ATOXICO) PS 0-1 DETERMINAR PD-L1?? TOXICIDAD SERIA INMUNOMEDIADA:

65 RECORDAR QUE EN EL Checkmate-067 ESTUDIO 3 BRAZOS CON IPI + NIVO, EL PUNTO DE CORTE ERA 5%
66 PDL-1: Expert opinion Overall, most trials (either retrospective or prospective) PD-L1 status have shown trends for increased response rates to PD-1 blockade in PD-L1 "positive" tumors (+ longer PFS, and longer overall survival compared with tumors that did not express PD-L1) BUT patients PDL-1 negative had too good responses with nivolumab in other trials, and near the same survival For melanoma, PD-L1 shouldn t determine whether we give nivolumab monotherapy, Regardless of PD-L1 status, you live longer with nivolumab. After the results of Checkmate-067, only if you are considering combination of Ipilimumab + nivolumab, it would be important to know PDL-1 Status. However, patients with high-risk characteristics, for which a rapid response is needed, should receive a combination of nivolumab and ipilimumab nevertheless PDL1-Status?. (?)

67
68 RECOMENDACIONES DE EXPERTOS: CASOS CLINICOS INMUNOTERAPIA?
69 Treatment of a Pt With Regional In-Transit Disease A 73-yr-old man previously treated for ulcerated melanoma on his sole, and subsequently with cryotherapy for in-transit lesions now presents with multiple new lesions but no evidence of distant metastatic disease Workup: BRAF WT, ECOG PS 0, LDH normal Expert recommendations Expert 1 Expert 2 Nivo or Pembro Ipi + Nivo Expert 3 Expert 4 Nivo or Pembro Nivo or Pembro Expert 5 Pembro Slide credit: clinicaloptions.com
70 Caso clinico 2: Paciente que va bien SIN INMUNOTERAPIA 85 AÑOS (HTA Y osteoporosis) Histerectomia x miomas. MELANOMA MALIGNO MID (extirpado jun-2010) (a los 78 años) Exéresis local (1/06/10): AP: melanoma maligno nodular, ulcerado, Breslow de 7 mm TC craneal y TAP (17/06/10): en FID imagen de defecto de repleción en ileón distal con imagen de masa de 2cm en la válvula ileocecal, ((1º COLONO DIC-2010: Melanosis coli, sin otras alts). Ampliación e injerto (30/06/10): AP: melanoma maligno nodular, quedando a menos de 1 mm del otro extremo de resección. NO SE HIZO BSGC X EDAD.
. RECHAZO AMPUTACION Y TTO INTRAARTERIAL QT PALIATIVA DTIC (reducción 20% inicial por edad) de oct-2010 a marzo-2011 x 8 ciclos.")
71 Caso clinico (2) SEPT-2010: APARICION DE LESIONES SATÉLITES, PET-TC (6/09/10): aumento del metabolismo solo en 1/3 inferior MID ; sin enfermedad a distancia. PAAF ADENOPATIA INGUINALES (-). Estadio clínico: pt4acn2cm0 (IIIB). RECHAZO AMPUTACION Y TTO INTRAARTERIAL QT PALIATIVA DTIC (reducción 20% inicial por edad) de oct-2010 a marzo-2011 x 8 ciclos. Toxic: náuseas G1, Astenia marcada, disgeusia. - Respuesta: Leve MEJORIA DE LAS LESIONES CUTANEAS, QUE FUERON DESAPARECIENDO (aplanándose, quedando como una peca residual) en los MESES SIGUIENTES
72 Caso clinico (3) evolucion Anticoagulada en marzo 2012 x FA Desde mayo-2012 precisó transfusión por anemia progresiva desde inicio de Sintrom + SOH (+ 3 muestras), COLONOSCOPIA ( ) TUMORACION POLIPOIDEA ADYACENTE A VALV. ILEOCECAL de unos 3 cm (AP. Mts de melanoma) TAC (dic-2012) SIN CAMBIOS (EN LA IMAGEN QUE SE ATRIBUIA A LIPOMA DESDE EL DGº EN 2010) CUTANIDES MID SEGUIAN EN REMISION. CIRUGIA: 8/2/13 Hemicolectomia derecha. (AP: MTS DE MELANOMA) ENERO-2017 NO HAY PROGRESION DE CUTANIDES NI RECAIDA DE ENFERMEDAD
73 INITIAL TREATMENT of a Pt With Metastatic Melanoma A 47-yr-old woman was recently diagnosed with stage IV melanoma with multiple liver, lung, and bone metastases; she is symptomatic with mild bone pain which she manages with daily acetaminophen Expert recommendations: BRAF Wild Type (ECOG PS 1, LDH normal) Expert 1 Expert 2 Expert 3 Expert 4 Expert 5 Ipi + Nivo Ipi + Nivo Ipi + Nivo Nivo or Pembro Pembro
74 INITIAL TREATMENT of a Pt With Metastatic Melanoma A 47-yr-old woman was recently diagnosed with stage IV melanoma with multiple liver, lung, and bone metastases; she is symptomatic with mild bone pain which she manages with daily acetaminophen Expert recommendations: BRAF Wild Type (ECOG PS 1, LDH normal) Expert 1 Expert 2 Expert 3 Expert 4 Expert 5 Ipi + Nivo Ipi + Nivo Ipi + Nivo Nivo or Pembro Pembro BRAF V600 Mutant (ECOG PS 1, LDH normal) Expert 1 Expert 2 Expert 3 Expert 4 Expert 5 Ipi + Nivo Ipi + Nivo Ipi + Nivo Nivo or Pembro Pembro
75 Initial Treatment of a Pt with Metastatic Melanoma and ECOG PS of 2 A 47-yr-old woman was recently diagnosed with stage IV melanoma with multiple liver, lung, and bone metastases; she is symptomatic with an ECOG PS of 2 Expert recommendations: BRAF Wild Type (ECOG PS 2, LDH high) Expert 1 Expert 2 Expert 3 Expert 4 Expert 5 Ipi + Nivo Ipi + Nivo Ipi + Nivo Nivo or Pembro Pembro Slide credit: clinicaloptions.com
76 Initial Treatment of a Pt with Metastatic Melanoma and ECOG PS of 2 A 47-yr-old woman was recently diagnosed with stage IV melanoma with multiple liver, lung, and bone metastases; she is symptomatic with an ECOG PS of 2 Expert recommendations: BRAF Wild Type (ECOG PS 2, LDH high) Expert 1 Expert 2 Expert 3 Expert 4 Expert 5 Ipi + Nivo Ipi + Nivo Ipi + Nivo Nivo or Pembro Pembro BRAF V600 Mutant (ECOG PS 2, LDH high) Expert 1 Expert 2 Expert 3 Expert 4 Expert 5 Dabrafenib + trametinib Dabrafenib + trametinib Ipi + Nivo Dabrafenib + trametinib Dabrafenib + trametinib Slide credit: clinicaloptions.com
77 PROGRESSION after First-line Anti PD-1 Therapy The PREVIOUS 47-yr-old pt elected to be treated with pembrolizumab; she does well with a PR, but 15 mos later, her condition worsens and scans show progression BRAF V600 Mutant (ECOG PS 1, LDH high) Expert 1 Expert 2 Expert 3 Expert 4 Expert 5 Dabrafenib + trametinib Dabrafenib + trametinib Dabrafenib + trametinib Dabrafenib + trametinib Dabrafenib + trametinib Slide credit: clinicaloptions.com
78 PROGRESSION after First-line Anti PD-1 Therapy The PREVIOUS 47-yr-old pt elected to be treated with pembrolizumab; she does well with a PR, but 15 mos later, her condition worsens and scans show progression BRAF Wild Type (ECOG PS 1, LDH high) Expert 1 Expert 2 Expert 3 Expert 4 Expert 5 Ipi Ipi + Nivo Ipi + Nivo Ipi Ipi BRAF V600 Mutant (ECOG PS 1, LDH high) Expert 1 Expert 2 Expert 3 Expert 4 Expert 5 Dabrafenib + trametinib Dabrafenib + trametinib Dabrafenib + trametinib Dabrafenib + trametinib Dabrafenib + trametinib Slide credit: clinicaloptions.com NO TENEMOS DATOS EN ESTE ESCENARIO
79 CheckMate-064: Sequential Treatment With Ipi and Nivo in Advanced Melanoma Randomized phase II trial Unresectable, stage III or IV melanoma; 1 prior systemic treatment for advanced disease; ECOG PS 0-1 (N = 140) Nivo 3 mg/kg q2w for 6 cycles (n = 70) Ipi 3 mg/kg q4w for 4 cycles Ipi 3 mg/kg q4w for 4 cycles (n = 70) Nivo 3 mg/kg q2w for 6 cycles Induction 1 Induction 2 Nivo 3 mg/kg q2w until progression/ unacceptable toxicity Primary endpoint: incidence of grade 3 AEs during induction Secondary endpoints: ORR (Wks 25 and 33), rate of PD (Wks 13 and 25) Hodi FS, et al. European Cancer Congress Abstract 23LBA. Slide credit: clinicaloptions.com
80 CheckMate-064: Results Incidence of treatment-related 3 AEs during induction Nivo Ipi (n = 68): 50.0% Ipi Nivo (n = 70): 42.9% No treatment-related deaths in either arm ORR at Wk 25 (all PR) Nivo Ipi (n = 68): 41.2% Ipi Nivo (n = 70): 20.0% Hodi FS, et al. European Cancer Congress Abstract 23LBA. Slide credit: clinicaloptions.com
81 Second line immunotherapy? Expert opinion Given the nearly identical structure, and clinical outcomes between pembrolizumab and nivolumab, there is no role in the clinical setting for transition from 1 monotherapy to this similar monotherapy An appropriate second-line consideration in this setting will be treatment with ipilimumab There have been no studies of ipilimumab for patients who have progressed while on PD-1. However, it is believed ipilimumab can be effective in some patients after progression while on PD-1. There have been no studies of combination of ipilimumab + nivolumab in this scenario
82 CONCLUSIONES (Uptodate) y MIAS ANTI PD1: PembrolizumabANTI PD1: Pembrolizumab and nivolumab, are the preferred immunotherapies in patients with advanced melanoma Ipilimumab, may retain a role in combination with anti-pd-1 antibodies at first line but with much greater toxicity Molecularly targeted therapy against the MAP kinase pathway is an important option of patients with a characteristic BRAF V600 mutation. The optimal sequencing of targeted therapy and immunotherapy has not been definitively established. For good PS patients without a V600 BRAF mutation, we recommend immunotherapy that includes an anti-pd-1 antibody rather than ipilimumab, high-dose IL-2 or chemotherapy (Grade 1A). The combination of nivolumabthe combination of nivolumab plus ipilimumab, if available, rather than an anti-pd-1 antibody as monotherapy Based its possible In high risk patients (Grade 2B) upon lower-level evidence, there is consensus that the intervention is appropriate.
83 Conclusiones (2) However, long-term follow up is still pending, which is needed to fully assess the benefit of PD-1 blockade Despite the low toxicity of PD-1 inhibitors, AEs can still be in rare cases severe and even lethal. Patients and treating physicians have to be aware of possible immune-related AEs and sufficient knowledge and experience The combination of PD-1 inhibitors and anti-ctla-4 antibody has just been approved and will also play a role in the future; it is still unclear in which patient population At present, it seems patients with PD-L1 negative tumors benefit most from the combination therapy. There are still a substantial number of patients who show innate resistance to any approved immunotherapy
84 Que necesitamos? SENTIDO COMUN Estudios de Grupos cooperativos, que respondan preguntas clínicas Definir el mejor tratamiento para cada paciente según factores pronósticos (de paciente y del tumor) Ensayos sobre duración de tratamientos con antipd1 (sostenibilidad del sistema de salud) Ensayos de tratamiento combinado (sucesivo) de terapias dirigidas?? (y en cuanto se obtenga respuesta mantenerla con inmunoterapia) Ensayos de inmunoterapia + quimioterapia?
85 . NO SER TALIBANES DE LA INMUNOTERAPIA "There is no better targeted therapy than to have a T cell that has a T-cell receptor that specifically recognizes a specific tumor antigen??" ANTONI RIBAS TB TENEMOS LA TERAPIA DIRIGIDA USEMOS AMBAS DE LA MEJOR MANERA POSIBLE

86 MUCHAS GRACIAS POR SU ATENCION
87 PUNTOS DE CONTROL PARA LA INMUNOTERAPIA Ganglio Tumor
88
Evolución de la supervivencia en melanoma metastásico BRAF mutado. Nuevas estrategias de tratamiento.
 Evolución de la supervivencia en melanoma metastásico BRAF mutado. Nuevas estrategias de tratamiento. Dra. Ainara Soria Rivas Servicio de Oncología Médica Hospital Ramón y Cajal Cuál es la supervivencia
Evolución de la supervivencia en melanoma metastásico BRAF mutado. Nuevas estrategias de tratamiento. Dra. Ainara Soria Rivas Servicio de Oncología Médica Hospital Ramón y Cajal Cuál es la supervivencia
Terapias anti PD1- PDL1. Luis de la Cruz Merino Sº Oncología Médica. HUVMacarena (Sevilla)
") Terapias anti PD1- PDL1 Luis de la Cruz Merino Sº Oncología Médica. HUVMacarena (Sevilla) INDICE EL EJE PD1/PD-L1 Y LA SINAPSIS INMUNE ANTICUERPOS MONOCLONALES EN ESTUDIO DESARROLLO AC MO ANTI PD1 EN MELANOMA
Terapias anti PD1- PDL1 Luis de la Cruz Merino Sº Oncología Médica. HUVMacarena (Sevilla) INDICE EL EJE PD1/PD-L1 Y LA SINAPSIS INMUNE ANTICUERPOS MONOCLONALES EN ESTUDIO DESARROLLO AC MO ANTI PD1 EN MELANOMA
Qué hacemos con los pacientes B-RAF mutados? Alfonso Berrocal Hospital General Universitario, Valencia
 Qué hacemos con los pacientes B-RAF mutados? Alfonso Berrocal Hospital General Universitario, Valencia Ventajas y desventajas de la inmunoterapia Ventajas Pacientes Largos supervivientes Ipilimumab 20%
Qué hacemos con los pacientes B-RAF mutados? Alfonso Berrocal Hospital General Universitario, Valencia Ventajas y desventajas de la inmunoterapia Ventajas Pacientes Largos supervivientes Ipilimumab 20%
Terapia de campo de tumores en el tratamiento del glioblastoma
 Terapia de campo de tumores en el tratamiento del glioblastoma Revisión sistemática Informe de síntesis de tecnología emergente Tumor treating fields therapy (TTF) for glioblastoma. A Systematic Review
Terapia de campo de tumores en el tratamiento del glioblastoma Revisión sistemática Informe de síntesis de tecnología emergente Tumor treating fields therapy (TTF) for glioblastoma. A Systematic Review
El Inmunomomento en Melanoma: Nivolumab más respuestas y larga supervivencia? Alfonso Berrocal
 El Inmunomomento en Melanoma: Nivolumab más respuestas y larga supervivencia? Alfonso Berrocal Proporción vivos Supervivencia con Ipilumumab en acceso expandido 1.0 0.9 0.8 Mediana de supervivencia meses
El Inmunomomento en Melanoma: Nivolumab más respuestas y larga supervivencia? Alfonso Berrocal Proporción vivos Supervivencia con Ipilumumab en acceso expandido 1.0 0.9 0.8 Mediana de supervivencia meses
Cáncer de mama metastásico ER-/HER2+ y resistencia precoz a la terapia con trastuzumab
 Cáncer de mama metastásico ER-/HER2+ y resistencia precoz a la terapia con trastuzumab Eva M Ciruelos Gil Hospital Universitario 12 de Octubre, Madrid Caso clínico Paciente con cáncer de mama HER2+ y recidiva
Cáncer de mama metastásico ER-/HER2+ y resistencia precoz a la terapia con trastuzumab Eva M Ciruelos Gil Hospital Universitario 12 de Octubre, Madrid Caso clínico Paciente con cáncer de mama HER2+ y recidiva
Inmunoterapia del Melanoma Maligno: Rompiendo Barreras. Alfonso Berrocal Servicio Oncología Medica Hospital General de Valencia
 Inmunoterapia del Melanoma Maligno: Rompiendo Barreras Alfonso Berrocal Servicio Oncología Medica Hospital General de Valencia Avances por mejor conocimiento de la biología McArthur GA, Ribas A. J Clin
Inmunoterapia del Melanoma Maligno: Rompiendo Barreras Alfonso Berrocal Servicio Oncología Medica Hospital General de Valencia Avances por mejor conocimiento de la biología McArthur GA, Ribas A. J Clin
Cómo definen los Oncólogos Alta Carga Tumoral en Cáncer de Mama Metastásico?
 Cómo definen los Oncólogos Alta Carga Tumoral en Cáncer de Mama Metastásico? Consenso sobre Cáncer de Mama Agresivo Her2- en Primera línea de Quimioterapia Consenso sobre Cáncer de Mama Agresivo Her2-
Cómo definen los Oncólogos Alta Carga Tumoral en Cáncer de Mama Metastásico? Consenso sobre Cáncer de Mama Agresivo Her2- en Primera línea de Quimioterapia Consenso sobre Cáncer de Mama Agresivo Her2-
Futuro de las combinaciones (de inmunoterapia) en el tratamiento del melanoma avanzado
 en el tratamiento del melanoma avanzado") Futuro de las combinaciones (de inmunoterapia) en el tratamiento del melanoma avanzado Iván Márquez Rodas MD, PhD Servicio de Oncología Médica Hospital General Universitario Gregorio Marañón DISCLOSURES
Futuro de las combinaciones (de inmunoterapia) en el tratamiento del melanoma avanzado Iván Márquez Rodas MD, PhD Servicio de Oncología Médica Hospital General Universitario Gregorio Marañón DISCLOSURES
Terapias anti CTLA-4. Curso Básico de Inmunología e Inmunoterapia y cáncer. Alfonso Berrocal Hospital General Valencia
 Terapias anti CTLA-4 Curso Básico de Inmunología e Inmunoterapia y cáncer Alfonso Berrocal Hospital General Valencia Mecanismo de acción Teoría Tres señales: Co-estimulación Interacción B7/CD28 CD28 se
Terapias anti CTLA-4 Curso Básico de Inmunología e Inmunoterapia y cáncer Alfonso Berrocal Hospital General Valencia Mecanismo de acción Teoría Tres señales: Co-estimulación Interacción B7/CD28 CD28 se
Metástasis cerebrales
 Metástasis cerebrales Juan Antonio Verdún Aguilar Servicio de Oncología Médica del Complejo hospitalario de Navarra Introducción: La afectación a nivel cerebral es una complicación frecuente en el paciente
Metástasis cerebrales Juan Antonio Verdún Aguilar Servicio de Oncología Médica del Complejo hospitalario de Navarra Introducción: La afectación a nivel cerebral es una complicación frecuente en el paciente
Tratamiento inmunoterápico de las metástasis cerebrales. Alfonso Berrocal Hospital General de Valencia
 Tratamiento inmunoterápico de las metástasis cerebrales Alfonso Berrocal Hospital General de Valencia Inmunidad y metástasis cerebrales Cancer 2013;119:2737-46. Ipilimumab y metástasis SNC Ipilimumab bloquea
Tratamiento inmunoterápico de las metástasis cerebrales Alfonso Berrocal Hospital General de Valencia Inmunidad y metástasis cerebrales Cancer 2013;119:2737-46. Ipilimumab y metástasis SNC Ipilimumab bloquea
Base de Datos Carcinoides Bronquiales
 Base de Datos Carcinoides Bronquiales Justificación Neoplasias de estirpe neuroendocrina y asiento pulmonar Yao JC, et al. J Clin Oncol 2008:26;3063-3072 Justificación 35.825 casos (1973-2004) % Primario
Base de Datos Carcinoides Bronquiales Justificación Neoplasias de estirpe neuroendocrina y asiento pulmonar Yao JC, et al. J Clin Oncol 2008:26;3063-3072 Justificación 35.825 casos (1973-2004) % Primario
MELANOMA MESA REDONDA 4 DEFINIENDO LA SECUENCIA ÓPTIMA DE TRATAMIENTO EN CÁNCER AVANZADO
 MESA REDONDA 4 DEFINIENDO LA SECUENCIA ÓPTIMA DE TRATAMIENTO EN CÁNCER AVANZADO MELANOMA Salvador Martín Algarra Clínica Universidad de Navarra Pamplona En los últimos años ha habido considerables avances
MESA REDONDA 4 DEFINIENDO LA SECUENCIA ÓPTIMA DE TRATAMIENTO EN CÁNCER AVANZADO MELANOMA Salvador Martín Algarra Clínica Universidad de Navarra Pamplona En los últimos años ha habido considerables avances
OPTIMIZACIÓN TRATAMIENTO ANTI-EGFR. Ruth Vera Oncología Médica
 OPTIMIZACIÓN TRATAMIENTO ANTI-EGFR Ruth Vera Oncología Médica OPTIMIZACIÓN TRATAMIENTO anti-egfr OPTIMIZAR quiere decir: Buscar los mejores resultados Planificar una actividad para obtener los mejores
OPTIMIZACIÓN TRATAMIENTO ANTI-EGFR Ruth Vera Oncología Médica OPTIMIZACIÓN TRATAMIENTO anti-egfr OPTIMIZAR quiere decir: Buscar los mejores resultados Planificar una actividad para obtener los mejores
IPILIMUMAB EN AVANZADO/METASTASICO
 IPILIMUMAB EN MELANOMA AVANZADO/METASTASICO GROWING UP IN ONCOLOGY Sesión 19 de junio de 2012 REBECA ALCALDE PAMPLIEGA R4 ONCOLOGIA MEDICA HOSPITAL UNIVERSITARIO RAMÓN Y CAJAL QUÉ ES IPILIMUMAB? Anticuerpo
IPILIMUMAB EN MELANOMA AVANZADO/METASTASICO GROWING UP IN ONCOLOGY Sesión 19 de junio de 2012 REBECA ALCALDE PAMPLIEGA R4 ONCOLOGIA MEDICA HOSPITAL UNIVERSITARIO RAMÓN Y CAJAL QUÉ ES IPILIMUMAB? Anticuerpo
Cáncer de vejiga. Qué hemos aprendido estos últimos años? Begoña Mellado Hospital Clínic. Barcelona
 Cáncer de vejiga Qué hemos aprendido estos últimos años? Begoña Mellado Hospital Clínic. Barcelona Qué hemos aprendido estos últimos años de cáncer de vejiga? Tratamiento adyuvante/neoadyuvante Enfermedad
Cáncer de vejiga Qué hemos aprendido estos últimos años? Begoña Mellado Hospital Clínic. Barcelona Qué hemos aprendido estos últimos años de cáncer de vejiga? Tratamiento adyuvante/neoadyuvante Enfermedad
Metástasis SNC papel tratamiento sistémico. Dra Ana Arance Hospital Clínic Barcelona
 Metástasis SNC papel tratamiento sistémico Dra Ana Arance Hospital Clínic Barcelona MELANOMA: METÁSTASIS CEREBRALES Melanoma Metastásico: 20% presentan M1 SNC 50% desarrollarán M1 SNC 55-75% autopsias
Metástasis SNC papel tratamiento sistémico Dra Ana Arance Hospital Clínic Barcelona MELANOMA: METÁSTASIS CEREBRALES Melanoma Metastásico: 20% presentan M1 SNC 50% desarrollarán M1 SNC 55-75% autopsias
INMUNOTERAPIA EN CÁNCER DE CABEZA Y CUELLO. JULIO LAMBEA SORROSAL Servicio de Oncología Médica CLÍNICO LOZANO BLESA ZARAGOZA
 INMUNOTERAPIA EN CÁNCER DE CABEZA Y CUELLO JULIO LAMBEA SORROSAL Servicio de Oncología Médica CLÍNICO LOZANO BLESA ZARAGOZA HISTORIA DEL TRATAMIENTO DE LOS TUMORES DE CABEZA Y CUELLO 2 HISTORIA DEL TRATAMIENTO
INMUNOTERAPIA EN CÁNCER DE CABEZA Y CUELLO JULIO LAMBEA SORROSAL Servicio de Oncología Médica CLÍNICO LOZANO BLESA ZARAGOZA HISTORIA DEL TRATAMIENTO DE LOS TUMORES DE CABEZA Y CUELLO 2 HISTORIA DEL TRATAMIENTO
Novedad en el tratamiento del cáncer diferenciado de tiroides: Lenvatinib. Dra. T. Ramón y Cajal Hospital Sant Pau
 Novedad en el tratamiento del cáncer diferenciado de tiroides: Lenvatinib Dra. T. Ramón y Cajal Hospital Sant Pau Incidencia y mortalidad Incidencia creciente 12ª causa tumor sólido mujer 17ª causa tumor
Novedad en el tratamiento del cáncer diferenciado de tiroides: Lenvatinib Dra. T. Ramón y Cajal Hospital Sant Pau Incidencia y mortalidad Incidencia creciente 12ª causa tumor sólido mujer 17ª causa tumor
Cómo modificará la Inmunoterapia el panorama de tratamiento del cáncer? Dra Ana Arance Oncología Médica Hospital Clínic Barcelona
 Cómo modificará la Inmunoterapia el panorama de tratamiento del cáncer? Dra Ana Arance Oncología Médica Hospital Clínic Barcelona The Cancer-Immunity Cycle Chen et al. Immunity 39, July 25, 2013 Factores
Cómo modificará la Inmunoterapia el panorama de tratamiento del cáncer? Dra Ana Arance Oncología Médica Hospital Clínic Barcelona The Cancer-Immunity Cycle Chen et al. Immunity 39, July 25, 2013 Factores
ALTERNATIVAS: 2ª Línea y posteriores. Dra. Ruth Vera Servicio Oncología Médica Complejo Hospitalario de Navarra
 ALTERNATIVAS: 2ª Línea y posteriores Dra. Ruth Vera Servicio Oncología Médica Complejo Hospitalario de Navarra 1. INTRODUCCIÓN 2. TRATAMIENTO DE SEGUNDA LÍNEA CON TERAPIAS ANTIEGFR 1. TRATAMIENTO DE SEGUNDA
ALTERNATIVAS: 2ª Línea y posteriores Dra. Ruth Vera Servicio Oncología Médica Complejo Hospitalario de Navarra 1. INTRODUCCIÓN 2. TRATAMIENTO DE SEGUNDA LÍNEA CON TERAPIAS ANTIEGFR 1. TRATAMIENTO DE SEGUNDA
Agentes dirigidos frente al hueso
 Agentes dirigidos frente al hueso IDEAS PRINCIPALES 2. Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, et al. Design and end points of clinical trials for patients with progressive
Agentes dirigidos frente al hueso IDEAS PRINCIPALES 2. Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, et al. Design and end points of clinical trials for patients with progressive
Alternativas de tratamiento de segunda línea postdocetaxel en Cáncer de Próstata en progresión con niveles de castración de testosterona (CPRC)
") Alternativas de tratamiento de segunda línea postdocetaxel en Cáncer de Próstata en progresión con niveles de castración de testosterona (CPRC) Dr Pablo Maroto Oncología Médica, Hospital de Sant Pau El
Alternativas de tratamiento de segunda línea postdocetaxel en Cáncer de Próstata en progresión con niveles de castración de testosterona (CPRC) Dr Pablo Maroto Oncología Médica, Hospital de Sant Pau El
PATOLOGIA MOLECULAR DEL CARCINOMA DE COLON. Eva Musulén
 PATOLOGIA MOLECULAR DEL CARCINOMA DE COLON Eva Musulén Patología molecular del CCR 1. Identificar pacientes de riesgo (Síndrome de Lynch) Inestabilidad de microsatélites 2. Guiar estrategia terapéutica
PATOLOGIA MOLECULAR DEL CARCINOMA DE COLON Eva Musulén Patología molecular del CCR 1. Identificar pacientes de riesgo (Síndrome de Lynch) Inestabilidad de microsatélites 2. Guiar estrategia terapéutica
Estudio SHARP. Implicaciones en la Prevención 2ª de la Cardiopatía Isquémica. José R. González Juanatey
 Estudio SHARP 1 Implicaciones en la Prevención 2ª de la Cardiopatía Isquémica 1 José R. González Juanatey Área Cardiovascular. Hospital Clínico Universitario de Santiago de Compostela Ezetimibe 2011 Cuestiones
Estudio SHARP 1 Implicaciones en la Prevención 2ª de la Cardiopatía Isquémica 1 José R. González Juanatey Área Cardiovascular. Hospital Clínico Universitario de Santiago de Compostela Ezetimibe 2011 Cuestiones
Bevacizumab en Cáncer de Colon
 1 Bevacizumab ONCOLOGÍA en Cáncer de Colon 2013 Bevacizumab en Cáncer de Colon Recomendaciones para su Uso Coordinador: Dr. Esteban Lifschitz Autores: Dr. Patricio Servienti, Dr. Ventura Simonovich Evaluación
1 Bevacizumab ONCOLOGÍA en Cáncer de Colon 2013 Bevacizumab en Cáncer de Colon Recomendaciones para su Uso Coordinador: Dr. Esteban Lifschitz Autores: Dr. Patricio Servienti, Dr. Ventura Simonovich Evaluación
GEICAM y su compromisocon la investigaciónliderando el desarrollode los inhibidorescdk4/6
 GEICAM y su compromisocon la investigaciónliderando el desarrollode los inhibidorescdk4/6 Agusti Barnadas Servicio de Oncologia Médica Hospital Sant Pau Barcelona El contenido de esta presentación refleja
GEICAM y su compromisocon la investigaciónliderando el desarrollode los inhibidorescdk4/6 Agusti Barnadas Servicio de Oncologia Médica Hospital Sant Pau Barcelona El contenido de esta presentación refleja
ESTUDIO DE BIOMARCADORES Y VALOR CLÍNICO DE LA BIOPSIA LÍQUIDA EN MELANOMA
 ESTUDIO DE BIOMARCADORES Y VALOR CLÍNICO DE LA BIOPSIA LÍQUIDA EN MELANOMA José Luis Rodríguez Peralto HOSPITAL 12 DE OCTUBRE, MADRID GENOMIC CHANGES IN THE NUMBER OF DNA COPIES IN DIFFERENTS SUBTYPES
ESTUDIO DE BIOMARCADORES Y VALOR CLÍNICO DE LA BIOPSIA LÍQUIDA EN MELANOMA José Luis Rodríguez Peralto HOSPITAL 12 DE OCTUBRE, MADRID GENOMIC CHANGES IN THE NUMBER OF DNA COPIES IN DIFFERENTS SUBTYPES
Lucía Teijeira Sánchez Oncología médica Complejo Hospitalario de Navarra
 Terapias dirigidas en el anciano Lucía Teijeira Sánchez Oncología médica Complejo Hospitalario de Navarra Epidemiología Definiciones Qué es paciente anciano? No es lo mismo que paciente frágil No es lo
Terapias dirigidas en el anciano Lucía Teijeira Sánchez Oncología médica Complejo Hospitalario de Navarra Epidemiología Definiciones Qué es paciente anciano? No es lo mismo que paciente frágil No es lo
Nuevas Estrategias con Inhibidores de Puntos de Control Celular en Linfomas de Hodgkin
 Nuevas Estrategias con Inhibidores de Puntos de Control Celular en Linfomas de Hodgkin Dra. María Alejandra Torres Viera Hematología Oncología 360, Caracas Caracas, Marzo 2016!" LH: Sobrevida De Acuerdo
Nuevas Estrategias con Inhibidores de Puntos de Control Celular en Linfomas de Hodgkin Dra. María Alejandra Torres Viera Hematología Oncología 360, Caracas Caracas, Marzo 2016!" LH: Sobrevida De Acuerdo
XX JORNADA DE LA SOCIEDAD DE MEDICINA NUCLEAR E IMAGEN MOLECULAR DE VALENCIA Y MURCIA
 XX JORNADA DE LA SOCIEDAD DE MEDICINA NUCLEAR E IMAGEN MOLECULAR DE VALENCIA Y MURCIA Dra Virtudes Soriano Fundación Instituto Valenciano de Oncologia Valencia 29 de Abril 2016 HISTORIA INMUNOTERAPIA EN
XX JORNADA DE LA SOCIEDAD DE MEDICINA NUCLEAR E IMAGEN MOLECULAR DE VALENCIA Y MURCIA Dra Virtudes Soriano Fundación Instituto Valenciano de Oncologia Valencia 29 de Abril 2016 HISTORIA INMUNOTERAPIA EN
Cetuximab: mucho más que un estándar en cáncer de cabeza y cuello. Alfonso Berrocal Hospital General Valencia
 Cetuximab: mucho más que un estándar en cáncer de cabeza y cuello Alfonso Berrocal Hospital General Valencia Indicaciones terapéuticas Cetuximab está indicado para el tratamiento de pacientes con cáncer
Cetuximab: mucho más que un estándar en cáncer de cabeza y cuello Alfonso Berrocal Hospital General Valencia Indicaciones terapéuticas Cetuximab está indicado para el tratamiento de pacientes con cáncer
CÁNCER GÁSTRICO AVANZADO: ALTERNATIVAS EN SEGUNDA LÍNEA. Fernando Rivera Herrero Sv Oncología Médica HU M Valdecilla. Santander
 CÁNCER GÁSTRICO AVANZADO: ALTERNATIVAS EN SEGUNDA LÍNEA Fernando Rivera Herrero Sv Oncología Médica HU M Valdecilla. Santander Cáncer Gástrico Avanzado: alternativas en 2ª línea Varios estándares en 1ª
CÁNCER GÁSTRICO AVANZADO: ALTERNATIVAS EN SEGUNDA LÍNEA Fernando Rivera Herrero Sv Oncología Médica HU M Valdecilla. Santander Cáncer Gástrico Avanzado: alternativas en 2ª línea Varios estándares en 1ª
DABRAFENIB en el tratamiento dea melanoma INFORME CFT- HOSPITAL REINA SOFÍA CÓRDOBA
 DABRAFENIB en el tratamiento dea melanoma INFORME CFT- HOSPITAL REINA SOFÍA CÓRDOBA 1.- Identificación del fármaco: Nombre Genérico: Dabrafenib Nombre Comercial: Tafinlar Presentaciones: E/28 comp 50 y
DABRAFENIB en el tratamiento dea melanoma INFORME CFT- HOSPITAL REINA SOFÍA CÓRDOBA 1.- Identificación del fármaco: Nombre Genérico: Dabrafenib Nombre Comercial: Tafinlar Presentaciones: E/28 comp 50 y
José Luis Pérez Gracia Departamento de Oncología Clínica Universidad de Navarra Madrid, 20 de noviembre de 2014
 Inmunoterapia en cáncer renal y futuro de las combinaciones con TKI José Luis Pérez Gracia Departamento de Oncología Clínica Universidad de Navarra Madrid, 20 de noviembre de 2014 Steps leading to an anti
Inmunoterapia en cáncer renal y futuro de las combinaciones con TKI José Luis Pérez Gracia Departamento de Oncología Clínica Universidad de Navarra Madrid, 20 de noviembre de 2014 Steps leading to an anti
Melanoma metastásico
 Selección del tratamiento en el melanoma maligno metastásico. Controversias y recomendaciones José Antonio López Martín HU 12 de Octubre- Madrid Melanoma: Melanoma metastásico Incidencia global en ascenso
Selección del tratamiento en el melanoma maligno metastásico. Controversias y recomendaciones José Antonio López Martín HU 12 de Octubre- Madrid Melanoma: Melanoma metastásico Incidencia global en ascenso
Everolimus más exemestano en pacientes con cáncer de mama avanzado ER+ HER2-
 Everolimus más exemestano en pacientes con cáncer de mama avanzado ER+ HER2- Dr E. Ciruelos Servicio Oncología Médica, Hospital Universitario 12 de Octubre Universidad Complutense, Madrid Grupo SOLTI de
Everolimus más exemestano en pacientes con cáncer de mama avanzado ER+ HER2- Dr E. Ciruelos Servicio Oncología Médica, Hospital Universitario 12 de Octubre Universidad Complutense, Madrid Grupo SOLTI de
Cáncer colorrectal metastático cómo decidir la mejor secuencia de tratamiento? Cristina Grávalos Hospital Universitario Marqués de Valdecilla
 Cáncer colorrectal metastático cómo decidir la mejor secuencia de tratamiento? Cristina Grávalos Hospital Universitario Marqués de Valdecilla Introducción - Cáncer colorrectal en España en el año 2012
Cáncer colorrectal metastático cómo decidir la mejor secuencia de tratamiento? Cristina Grávalos Hospital Universitario Marqués de Valdecilla Introducción - Cáncer colorrectal en España en el año 2012
Introducción al test molecular DecisionDx-MELANOMA
 i Introducción al test molecular DecisionDx-MELANOMA El primer test genético de pronóstico validado para pacientes con melanoma cutáneo en estadios iniciales I y II 1. Datos clínicos 2. Nuestra solución:
i Introducción al test molecular DecisionDx-MELANOMA El primer test genético de pronóstico validado para pacientes con melanoma cutáneo en estadios iniciales I y II 1. Datos clínicos 2. Nuestra solución:
Combinaciones Quimioterápicas en Hemopatías Malignas. Linfoma de Hodgkin
 Combinaciones Quimioterápicas en Hemopatías Malignas. Linfoma de Hodgkin Anna Sureda Servei d Hematologia Institut Catala d Oncologia Hospital Duran i Reynals Barcelona Tratamiento Antineoplásico en Hematología:
Combinaciones Quimioterápicas en Hemopatías Malignas. Linfoma de Hodgkin Anna Sureda Servei d Hematologia Institut Catala d Oncologia Hospital Duran i Reynals Barcelona Tratamiento Antineoplásico en Hematología:
Análisis de la coestimulación vía CD28 en células linfoides de pacientes infectados. con el virus de la Hepatitis C RESUMEN
 Análisis de la coestimulación vía CD28 en células linfoides de pacientes infectados con el virus de la Hepatitis C RESUMEN La infección por el virus de la hepatitis C (VHC) afecta a más de 170 millones
Análisis de la coestimulación vía CD28 en células linfoides de pacientes infectados con el virus de la Hepatitis C RESUMEN La infección por el virus de la hepatitis C (VHC) afecta a más de 170 millones
Cáncer de Riñón Avanzado (CRm) A quien y con que tratar en 3ª Línea
 A quien y con que tratar en 3ª Línea") Cáncer de Riñón Avanzado (CRm) A quien y con que tratar en 3ª Línea Hospital Universitario Central de Asturias Servicio de Oncología Médica Emilio Esteban González Cual de estas afirmaciones es más correcta
Cáncer de Riñón Avanzado (CRm) A quien y con que tratar en 3ª Línea Hospital Universitario Central de Asturias Servicio de Oncología Médica Emilio Esteban González Cual de estas afirmaciones es más correcta
Tratamiento adyuvante del melanoma de alto riesgo. Alfonso Berrocal Hospital General Universitario
 Tratamiento adyuvante del melanoma de alto riesgo Alfonso Berrocal Hospital General Universitario Necesidad de tratamiento Balch CM et al. JCO 2009: 6199-6206 Necesidad de nuevos tratamientos DFS SG Mejorado
Tratamiento adyuvante del melanoma de alto riesgo Alfonso Berrocal Hospital General Universitario Necesidad de tratamiento Balch CM et al. JCO 2009: 6199-6206 Necesidad de nuevos tratamientos DFS SG Mejorado
TAPCells BIOTECNOLOGÍA GLOBAL La Vacuna Chilena Contra el Melanoma. Prof. Dr. Flavio Salazar Onfray
 TAPCells BIOTECNOLOGÍA GLOBAL La Vacuna Chilena Contra el Melanoma Prof. Dr. Flavio Salazar Onfray MITO CHILE NO PRODUCE CIENCIA A NIVEL GLOBAL no SI! MELANOMA "THE MARKET" Melanoma is growing worldwide
TAPCells BIOTECNOLOGÍA GLOBAL La Vacuna Chilena Contra el Melanoma Prof. Dr. Flavio Salazar Onfray MITO CHILE NO PRODUCE CIENCIA A NIVEL GLOBAL no SI! MELANOMA "THE MARKET" Melanoma is growing worldwide
Doble Bloqueo Vertical en Cáncer de Mama HER2-positivo. Dr. Antonio Llombart Cussac Hospital Arnau Vilanova, Valencia
 Doble Bloqueo Vertical en Cáncer de Mama HER2-positivo Dr. Antonio Llombart Cussac Hospital Arnau Vilanova, Valencia CMM HER2[+]: Doble Bloqueo Vertical en 2014 Trastuzumab (T) es la terapia de elección
Doble Bloqueo Vertical en Cáncer de Mama HER2-positivo Dr. Antonio Llombart Cussac Hospital Arnau Vilanova, Valencia CMM HER2[+]: Doble Bloqueo Vertical en 2014 Trastuzumab (T) es la terapia de elección
Cáncer de mama luminal. Resistencia y nuevos fármacos Dr. Antonio Llombart. Hospital Universitari Arnau de Vilanova, Valencia
 Cáncer de mama luminal. Resistencia y nuevos fármacos Dr. Antonio Llombart. Hospital Universitari Arnau de Vilanova, Valencia Proportion without progression Primera línea en RH[+] IAs superiores a tamoxifeno
Cáncer de mama luminal. Resistencia y nuevos fármacos Dr. Antonio Llombart. Hospital Universitari Arnau de Vilanova, Valencia Proportion without progression Primera línea en RH[+] IAs superiores a tamoxifeno
El abordaje del carcinoma de células de Merkel
 El abordaje del carcinoma de células de Merkel Iván Márquez Rodas MD, PhD Servicio de Oncología Médica Hospital General Universitario Gregorio Marañón EPIDEMIOLOGÍA, PATOLOGÍA Y DIAGNÓSTICO LA IMPORTANCIA
El abordaje del carcinoma de células de Merkel Iván Márquez Rodas MD, PhD Servicio de Oncología Médica Hospital General Universitario Gregorio Marañón EPIDEMIOLOGÍA, PATOLOGÍA Y DIAGNÓSTICO LA IMPORTANCIA
Multidisciplinary Approach to Brain Metastasis from Melanoma
 Multidisciplinary Approach to Brain Metastasis from Melanoma -Local Therapies for Central Nervous System Metastases. -The Emerging Role of Systemic Therapies. Servicio de Hematología y Oncología Hospital
Multidisciplinary Approach to Brain Metastasis from Melanoma -Local Therapies for Central Nervous System Metastases. -The Emerging Role of Systemic Therapies. Servicio de Hematología y Oncología Hospital
Cetuximab en Cáncer de Colon
 1 Cetuximab ONCOLOGÍA en Cáncer de Colon 2013 Cetuximab en Cáncer de Colon Recomendaciones para su Uso Coordinador: Dr. Esteban Lifschitz Autores: Dr. Patricio Servienti, Dr. Ventura Simonovich Evaluación
1 Cetuximab ONCOLOGÍA en Cáncer de Colon 2013 Cetuximab en Cáncer de Colon Recomendaciones para su Uso Coordinador: Dr. Esteban Lifschitz Autores: Dr. Patricio Servienti, Dr. Ventura Simonovich Evaluación
La angiogénesis como factor clave en el tratamiento del cáncer renal tras progresión a un antiangiogénico previo
 La angiogénesis como factor clave en el tratamiento del cáncer renal tras progresión a un antiangiogénico previo Pablo Gajate Borau Oncología Médica Hospital Ramón y Cajal Importancia de la angiogenesis
La angiogénesis como factor clave en el tratamiento del cáncer renal tras progresión a un antiangiogénico previo Pablo Gajate Borau Oncología Médica Hospital Ramón y Cajal Importancia de la angiogenesis
Uso de ipilimumab en pacientes con melanoma metastásico. Experiencia en el Hospital Médica Sur
 Gaceta Mexicana de Oncología. 2014;13(3):157-161 www.elsevier.es Artículo original Uso de ipilimumab en pacientes con melanoma metastásico. Experiencia en el Hospital Médica Sur José Manuel Ruiz-Morales
Gaceta Mexicana de Oncología. 2014;13(3):157-161 www.elsevier.es Artículo original Uso de ipilimumab en pacientes con melanoma metastásico. Experiencia en el Hospital Médica Sur José Manuel Ruiz-Morales
Estrategias de inmunoterapia en cáncer genitourinario
 Estrategias de inmunoterapia en cáncer genitourinario Iván Martínez Forero MD, PhD Hospital Pablo Tobón Uribe imforero@hptu.org.co imforero@alumni.unav.es Disclosure BMS-Speaker Contenido Respuesta inmune
Estrategias de inmunoterapia en cáncer genitourinario Iván Martínez Forero MD, PhD Hospital Pablo Tobón Uribe imforero@hptu.org.co imforero@alumni.unav.es Disclosure BMS-Speaker Contenido Respuesta inmune
Influencia de las dislipemias y de su tratamiento sobre el metabolismo de la glucosa, la función renal y miocárdica
 Influencia de las dislipemias y de su tratamiento sobre el metabolismo de la glucosa, la función renal y miocárdica Dr. Carlos Guijarro Unidad de Medicina Interna Universidad Rey Juan Carlos Dislipemias,
Influencia de las dislipemias y de su tratamiento sobre el metabolismo de la glucosa, la función renal y miocárdica Dr. Carlos Guijarro Unidad de Medicina Interna Universidad Rey Juan Carlos Dislipemias,
Avances en el tratamiento del melanoma metastásico. José Antonio López Martín HU 12 de Octubre- Madrid
 Avances en el tratamiento del melanoma metastásico. José Antonio López Martín HU 12 de Octubre- Madrid Melanoma metastásico - 2010 Incidencia global en ascenso Edad de inicio menor que otros tumores Mal
Avances en el tratamiento del melanoma metastásico. José Antonio López Martín HU 12 de Octubre- Madrid Melanoma metastásico - 2010 Incidencia global en ascenso Edad de inicio menor que otros tumores Mal
Innovación terapéutica en cáncer de pulmón. Dr A. Artal Hospital Universitario Miguel Servet Zaragoza
 Innovación terapéutica en cáncer de pulmón Dr A. Artal Hospital Universitario Miguel Servet Zaragoza NINTEDANIB INMUNOTERAPIA NINTEDANIB INMUNOTERAPIA Second line First line Study Intervention Target PFS,
Innovación terapéutica en cáncer de pulmón Dr A. Artal Hospital Universitario Miguel Servet Zaragoza NINTEDANIB INMUNOTERAPIA NINTEDANIB INMUNOTERAPIA Second line First line Study Intervention Target PFS,
La Inmunoterapia como tratamiento oncológico: Melanoma. Dr. Joaquín Fra Rodríguez Hospital Universitario Río Hortega Valladolid
 La Inmunoterapia como tratamiento oncológico: Melanoma Dr. Joaquín Fra Rodríguez Hospital Universitario Río Hortega Valladolid LA INMUNIDAD Y LA DISEMINACIÓN DE LOS TUMORES MALIGNOS Desarrollo de las metástasis
La Inmunoterapia como tratamiento oncológico: Melanoma Dr. Joaquín Fra Rodríguez Hospital Universitario Río Hortega Valladolid LA INMUNIDAD Y LA DISEMINACIÓN DE LOS TUMORES MALIGNOS Desarrollo de las metástasis
Tratamiento de la recai da del ca ncer de ovario en pacientes no candidatas a platino
 Tratamiento de la recai da del ca ncer de ovario en pacientes no candidatas a platino Ana Santaballa Bertrán, MD, PhD Servicio Oncologi a Me dica, Hospital Universitario y Polite cnico la Fe, Valencia
Tratamiento de la recai da del ca ncer de ovario en pacientes no candidatas a platino Ana Santaballa Bertrán, MD, PhD Servicio Oncologi a Me dica, Hospital Universitario y Polite cnico la Fe, Valencia
GLIOBLASTOMA TERAPIA ANTIANGIOGÉNICA. PERCEPCIÓN O REALIDAD.
 GLIOBLASTOMA TERAPIA ANTIANGIOGÉNICA. PERCEPCIÓN O REALIDAD. Juan M Sepúlveda Sánchez Noviembre 2012 Congreso Colombiano de Actualización en Hematología y Oncología PROGRESIÓN TRAS QUIMIORRADIOTERAPIA
GLIOBLASTOMA TERAPIA ANTIANGIOGÉNICA. PERCEPCIÓN O REALIDAD. Juan M Sepúlveda Sánchez Noviembre 2012 Congreso Colombiano de Actualización en Hematología y Oncología PROGRESIÓN TRAS QUIMIORRADIOTERAPIA
Linfomas Agresivos Tratamiento de 1ª Línea
 Conclusiones de The American Society of Hematology 54th Annual Meeting Linfomas Agresivos Tratamiento de 1ª Línea Javier Briones Hospital Santa Creu i Sant Pau. Barcelona Linfoma Difuso Células Grandes
Conclusiones de The American Society of Hematology 54th Annual Meeting Linfomas Agresivos Tratamiento de 1ª Línea Javier Briones Hospital Santa Creu i Sant Pau. Barcelona Linfoma Difuso Células Grandes
Abordaje del paciente frágil con cáncer de páncreas metastásico. Dr. Javier Sastre Servicio de Oncología HC San Carlos (Madrid)
") Abordaje del paciente frágil con cáncer de páncreas metastásico Dr. Javier Sastre Servicio de Oncología HC San Carlos (Madrid) Qué entendemos por paciente frágil? Concepto asociado a la senescencia: Cambio
Abordaje del paciente frágil con cáncer de páncreas metastásico Dr. Javier Sastre Servicio de Oncología HC San Carlos (Madrid) Qué entendemos por paciente frágil? Concepto asociado a la senescencia: Cambio
Expresión de PD-L1 como Factor Predictivo de Respuesta: Resultados Clínicos con Inmunoterapia Dolores Isla Servicio de Oncología Médica HCU Lozano
 Expresión de PD-L1 como Factor Predictivo de Respuesta: Resultados Clínicos con Inmunoterapia Dolores Isla Servicio de Oncología Médica HCU Lozano Blesa de Zaragoza Immune Checkpoint Inhibitors Biomarkers
Expresión de PD-L1 como Factor Predictivo de Respuesta: Resultados Clínicos con Inmunoterapia Dolores Isla Servicio de Oncología Médica HCU Lozano Blesa de Zaragoza Immune Checkpoint Inhibitors Biomarkers
Comisión Nacional del Mercado de Valores Att. Director del Área de Mercados C/ Edison, 4 28006 Madrid. Madrid, a 17 de septiembre de 2014
 Comisión Nacional del Mercado de Valores Att. Director del Área de Mercados C/ Edison, 4 28006 Madrid Madrid, a 17 de septiembre de 2014 De conformidad con lo previsto en el artículo 82 de la Ley del Mercado
Comisión Nacional del Mercado de Valores Att. Director del Área de Mercados C/ Edison, 4 28006 Madrid Madrid, a 17 de septiembre de 2014 De conformidad con lo previsto en el artículo 82 de la Ley del Mercado
Cáncer de Mama: Inhibidores de vía PI3K/Akt/mTOR, ciclinas, anti-ctla4 y anti PD1. Dr. Claudio Painemal D. Director Médico
 Cáncer de Mama: Inhibidores de vía PI3K/Akt/mTOR, ciclinas, anti-ctla4 y anti PD1 Dr. Claudio Painemal D. Director Médico PI3K/Akt/mTOR Frecuentemente activada en cáncer de mama PIK3CA es el gen más frecuentemente
Cáncer de Mama: Inhibidores de vía PI3K/Akt/mTOR, ciclinas, anti-ctla4 y anti PD1 Dr. Claudio Painemal D. Director Médico PI3K/Akt/mTOR Frecuentemente activada en cáncer de mama PIK3CA es el gen más frecuentemente
Recomendaciones para su uso
 1 Ipilimumab DERMATOLOGÍA en Melanoma 2013 Recomendaciones para su uso Coordinador: Dr. Esteban Lifschitz Autores: Dr. Mariano Marini, Dr. Ventura Simonovich 1 LOS AUTORES RECOMIENDAN QUE EN CASO DE ESTAR
1 Ipilimumab DERMATOLOGÍA en Melanoma 2013 Recomendaciones para su uso Coordinador: Dr. Esteban Lifschitz Autores: Dr. Mariano Marini, Dr. Ventura Simonovich 1 LOS AUTORES RECOMIENDAN QUE EN CASO DE ESTAR
NIVOLUMAB EN MELANOMA METASTÁSICO INFORME CFT- HOSPITAL REINA SOFÍA CÓRDOBA
 NIVOLUMAB EN MELANOMA METASTÁSICO INFORME CFT- HOSPITAL REINA SOFÍA CÓRDOBA 1.- Identificación del fármaco: Nombre Genérico: Nivolumab Nombre Comercial: Opdivo Presentaciones: E/1 Vial 10mg/ml de 4ml (40mg)
NIVOLUMAB EN MELANOMA METASTÁSICO INFORME CFT- HOSPITAL REINA SOFÍA CÓRDOBA 1.- Identificación del fármaco: Nombre Genérico: Nivolumab Nombre Comercial: Opdivo Presentaciones: E/1 Vial 10mg/ml de 4ml (40mg)
Avances y Retos en Oncologica. Manuel Hidalgo, M.D., Ph.D.
 Avances y Retos en Oncologica Manuel Hidalgo, M.D., Ph.D. Agenda Conocimiento basico. Prevencion. Diagnostico. Tratamiento. The Hallmarks of Cancer Hanahan and Weinberg, Cell 2000 Simplified view of EGFR
Avances y Retos en Oncologica Manuel Hidalgo, M.D., Ph.D. Agenda Conocimiento basico. Prevencion. Diagnostico. Tratamiento. The Hallmarks of Cancer Hanahan and Weinberg, Cell 2000 Simplified view of EGFR
QUÈ PASSA AMB LA RDT DE CADENES GANGLIONARS. Dra. Arancha Eraso Servei d Oncologia Radioteràpia
 QUÈ PASSA AMB LA RDT DE CADENES GANGLIONARS. Dra. Arancha Eraso Servei d Oncologia Radioteràpia Pre- ACOSOG Z0011 y MA.20 SUPRA I II Paciente cn1 o GC positivo IRRADIACIÓN CADENAS IRRADIACIÓN SUPRACLAVICULAR
QUÈ PASSA AMB LA RDT DE CADENES GANGLIONARS. Dra. Arancha Eraso Servei d Oncologia Radioteràpia Pre- ACOSOG Z0011 y MA.20 SUPRA I II Paciente cn1 o GC positivo IRRADIACIÓN CADENAS IRRADIACIÓN SUPRACLAVICULAR
CONSIDERACIONES CLINICAS DE MGMT
 CONSIDERACIONES CLINICAS DE MGMT Carme Balaña ICO Germans Trias i Pujol Institut Català d Oncologia TRATAMIENTO DE PRIMERA LÍNEA TTO SEGUNDA LINEA Efecto terapéutico reconocido Mejoría supervivencia Efectos
CONSIDERACIONES CLINICAS DE MGMT Carme Balaña ICO Germans Trias i Pujol Institut Català d Oncologia TRATAMIENTO DE PRIMERA LÍNEA TTO SEGUNDA LINEA Efecto terapéutico reconocido Mejoría supervivencia Efectos
Doble Bloqueo Horizontal. Juan R de la Haba-Rodríguez Hospital Universitario Reina Sofía. Córdoba
 Juan R de la Haba-Rodríguez Hospital Universitario Reina Sofía. Córdoba Pertuzumab Cixitumumab Trastuzumab/DM1 Pertuzumab MM-111 ADAM 17 inhibitors HSP90 Inhibitors HDAC inhibitors Everolimus Temsirolimus
Juan R de la Haba-Rodríguez Hospital Universitario Reina Sofía. Córdoba Pertuzumab Cixitumumab Trastuzumab/DM1 Pertuzumab MM-111 ADAM 17 inhibitors HSP90 Inhibitors HDAC inhibitors Everolimus Temsirolimus
Meningitis Tuberculosa y su Tratamiento Santiago Moreno Hospital Ramón y Cajal. IRYCIS. Madrid
 Taller UITB 2012 Barcelona, 19-20 de Noviembre de 2012 Meningitis Tuberculosa y su Tratamiento Santiago Moreno Hospital Ramón y Cajal. IRYCIS. Madrid Meningitis tuberculosa Importancia Presentación clínica
Taller UITB 2012 Barcelona, 19-20 de Noviembre de 2012 Meningitis Tuberculosa y su Tratamiento Santiago Moreno Hospital Ramón y Cajal. IRYCIS. Madrid Meningitis tuberculosa Importancia Presentación clínica
Quimioterapia en Cáncer de Vejiga. Dr. Ovidio Fernández Calvo Complejo Hospitalario Universitario Ourense
 Quimioterapia en Cáncer de Vejiga Dr. Ovidio Fernández Calvo Complejo Hospitalario Universitario Ourense Evolution of systemic therapy for urothelial cancer 1 Sternberg CN et al. Cancer 1989;64(12):2448
Quimioterapia en Cáncer de Vejiga Dr. Ovidio Fernández Calvo Complejo Hospitalario Universitario Ourense Evolution of systemic therapy for urothelial cancer 1 Sternberg CN et al. Cancer 1989;64(12):2448
SRS en Metástasis Cerebrales. Dr. Alvaro Luongo Gardi
 SRS en Metástasis Cerebrales Dr. Alvaro Luongo Gardi 40% de los pacientes con cancer desarrollarán MC La incidencia de MC se duplicó dada la mayor sobrevida de los pacientes. Por mejor tecnología, detección
SRS en Metástasis Cerebrales Dr. Alvaro Luongo Gardi 40% de los pacientes con cancer desarrollarán MC La incidencia de MC se duplicó dada la mayor sobrevida de los pacientes. Por mejor tecnología, detección
CASO CLINICO: TRATAMIENTO NEOADYUVANTE EN CANCER MAMA HER-2 + Anabel Ballesteros García Hospital Universitario de La Princesa
 CASO CLINICO: TRATAMIENTO NEOADYUVANTE EN CANCER MAMA HER-2 + Anabel Ballesteros García Hospital Universitario de La Princesa CASO CLINICO 1 Mujer de 35 años ANTECEDENTES PERSONALES: Linfoma de Hodgkin
CASO CLINICO: TRATAMIENTO NEOADYUVANTE EN CANCER MAMA HER-2 + Anabel Ballesteros García Hospital Universitario de La Princesa CASO CLINICO 1 Mujer de 35 años ANTECEDENTES PERSONALES: Linfoma de Hodgkin
Impacto de los factores de riesgo cardiovascular tradicionales en el lupus eritematoso sistémico
 Impacto de los factores de riesgo cardiovascular tradicionales en el lupus eritematoso sistémico Dr. José Mario Sabio UEAS. Servicio de Medicina Interna. Hospital Universitario Virgen de la Nieves. Granada.
Impacto de los factores de riesgo cardiovascular tradicionales en el lupus eritematoso sistémico Dr. José Mario Sabio UEAS. Servicio de Medicina Interna. Hospital Universitario Virgen de la Nieves. Granada.
AVANCES EN EL MANEJO DEL GLIOBLASTOMA MULTIFORME EVALUACIÓN DE LA RESPUESTA
 AVANCES EN EL MANEJO DEL GLIOBLASTOMA MULTIFORME EVALUACIÓN DE LA RESPUESTA Dr. Miquel Macià & Dra. Anna Lucas Oncología Radioterápica Unidad Funcional de Neuro-Oncología Institut Català d Oncologia. L
AVANCES EN EL MANEJO DEL GLIOBLASTOMA MULTIFORME EVALUACIÓN DE LA RESPUESTA Dr. Miquel Macià & Dra. Anna Lucas Oncología Radioterápica Unidad Funcional de Neuro-Oncología Institut Català d Oncologia. L
SESIONES INTERHOSPITALARIAS MADRILEÑAS DE CÁNCER DE MAMA
 SESIONES INTERHOSPITALARIAS MADRILEÑAS DE CÁNCER DE MAMA Novedades bibliográficas en cáncer de mama Tercer Trimestre 2012 Beyond ASCO Federico Longo Muñoz Servicio de Oncología Médica Hospital Universitario
SESIONES INTERHOSPITALARIAS MADRILEÑAS DE CÁNCER DE MAMA Novedades bibliográficas en cáncer de mama Tercer Trimestre 2012 Beyond ASCO Federico Longo Muñoz Servicio de Oncología Médica Hospital Universitario
ALIMENTACIÓN VEGETARIANA- VEGANA EN EL EMBARAZO
 ALIMENTACIÓN VEGETARIANA- VEGANA EN EL EMBARAZO AUTORES: BASILIO, Agustina BROSA, Mercedes CURTI, Nadia GABRIELLI, Julia DIRECTOR: Lic. LÓPEZ, Laura Ciudad Autónoma de Buenos Aires Noviembre 2016 RESUMEN
ALIMENTACIÓN VEGETARIANA- VEGANA EN EL EMBARAZO AUTORES: BASILIO, Agustina BROSA, Mercedes CURTI, Nadia GABRIELLI, Julia DIRECTOR: Lic. LÓPEZ, Laura Ciudad Autónoma de Buenos Aires Noviembre 2016 RESUMEN
Ipilimumab en Melanoma Recomendaciones para su uso
 SEMINARIO TALLER PROPUESTA DE GUÍA DE PRACTICAS CLÍNICAS DE PATOLOGÍAS TUTELADAS Patologías/Tecnologías Tuteladas Guía de Práctica Ipilimumab en Melanoma Recomendaciones para su uso Recomendaciones para
SEMINARIO TALLER PROPUESTA DE GUÍA DE PRACTICAS CLÍNICAS DE PATOLOGÍAS TUTELADAS Patologías/Tecnologías Tuteladas Guía de Práctica Ipilimumab en Melanoma Recomendaciones para su uso Recomendaciones para
Brain Tumors. Glioma Tumors
 Brain Tumors A tumor that starts and grows in the brain is called a primary brain tumor. Primary brain tumors get their name from the type of cell or the part of the brain where they start growing. A secondary
Brain Tumors A tumor that starts and grows in the brain is called a primary brain tumor. Primary brain tumors get their name from the type of cell or the part of the brain where they start growing. A secondary
Cáncer de próstata. Paradigmas que cambian en 2013, por Mauricio Lema Medina
 Cáncer de próstata Paradigmas que cambian en 2013, por Mauricio Lema Medina Nuevos paradigmas en cáncer de próstata (CaPr) Temario 1 2 3 4 5 USPSTF recomienda NO practicar tamizaje con PSA Observación,
Cáncer de próstata Paradigmas que cambian en 2013, por Mauricio Lema Medina Nuevos paradigmas en cáncer de próstata (CaPr) Temario 1 2 3 4 5 USPSTF recomienda NO practicar tamizaje con PSA Observación,
CASO CLINICO 2: TUMOR NEUROENDOCRINO NO FUNCIONANTE
 CASO CLINICO 2: TUMOR NEUROENDOCRINO NO FUNCIONANTE INTRODUCCION Paciente de 70 años al diagnóstico Antecedentes de HTA, bloqueo completo con implantación de marcapasos, histeroaexectomía por tuberculosis
CASO CLINICO 2: TUMOR NEUROENDOCRINO NO FUNCIONANTE INTRODUCCION Paciente de 70 años al diagnóstico Antecedentes de HTA, bloqueo completo con implantación de marcapasos, histeroaexectomía por tuberculosis
Now that we have the choices, wich antiplatelet drug is prefered prior to PCI in the elective and in the ACS patient?
 Now that we have the choices, wich antiplatelet drug is prefered prior to PCI in the elective and in the ACS patient? Dr Alejandro Martínez Sepúlveda Universidad Católica de Chile La inhibición plaquetaria
Now that we have the choices, wich antiplatelet drug is prefered prior to PCI in the elective and in the ACS patient? Dr Alejandro Martínez Sepúlveda Universidad Católica de Chile La inhibición plaquetaria
Volatilidad: Noviembre 2010 Futuros Frijol de Soya
 Observaciones Junio 09, 2010 1. La volatilidad tiene una tendencia a aumentar de Junio a Julio. 2. Este reporte sugiere que se debería considerar la implementación de estrategias largas con opciones en
Observaciones Junio 09, 2010 1. La volatilidad tiene una tendencia a aumentar de Junio a Julio. 2. Este reporte sugiere que se debería considerar la implementación de estrategias largas con opciones en
DEFINIENDO LA SECUENCIA ÓPTIMA DE TRATAMIENTO EN CÁNCER DE PRÓSTATA RESISTENTE A CASTRACIÓN
 DEFINIENDO LA SECUENCIA ÓPTIMA DE TRATAMIENTO EN CÁNCER DE PRÓSTATA RESISTENTE A CASTRACIÓN Rebeca Lozano Mejorada Hospital Clínico Universitario de Salamanca TIMELINE CÁNCER DE PRÓSTATA Cáncer de Próstata
DEFINIENDO LA SECUENCIA ÓPTIMA DE TRATAMIENTO EN CÁNCER DE PRÓSTATA RESISTENTE A CASTRACIÓN Rebeca Lozano Mejorada Hospital Clínico Universitario de Salamanca TIMELINE CÁNCER DE PRÓSTATA Cáncer de Próstata
Linfocitos T con receptores antigénicos quiméricos en la inmunoterapia del cáncer: el amanecer de una nueva era?
 Linfocitos T con receptores antigénicos quiméricos en la inmunoterapia del cáncer: el amanecer de una nueva era? Dr. Miguel Lozano Molero Jefe de Sección de Hemoterapia Servicio de Hemoterapia y Hemostasia
Linfocitos T con receptores antigénicos quiméricos en la inmunoterapia del cáncer: el amanecer de una nueva era? Dr. Miguel Lozano Molero Jefe de Sección de Hemoterapia Servicio de Hemoterapia y Hemostasia
SIHI México, S. de R.L. de C.V. Pricing Guide
 Pricing Guide Rates effective as of: October 1, 2016 Note: Rates are subject to change without prior notice. Rates are stated in Mexican Pesos unless otherwise specified. page 1 of 5 Table Of Contents
Pricing Guide Rates effective as of: October 1, 2016 Note: Rates are subject to change without prior notice. Rates are stated in Mexican Pesos unless otherwise specified. page 1 of 5 Table Of Contents
KEYTRUDA (pembrolizumab)
") I. Denominación Distintiva KEYTRUDA. II. Denominación Genérica Pembrolizumab. III. Forma Farmacéutica y Formulación Forma Farmacéutica: Solución. Fórmula: El frasco ámpula contiene: Pembrolizumab. 100
I. Denominación Distintiva KEYTRUDA. II. Denominación Genérica Pembrolizumab. III. Forma Farmacéutica y Formulación Forma Farmacéutica: Solución. Fórmula: El frasco ámpula contiene: Pembrolizumab. 100
La innovación como garantía de calidad asistencial: Cáncer de próstata
 La innovación como garantía de calidad asistencial: Cáncer de próstata Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Complutense University Associate Professor
La innovación como garantía de calidad asistencial: Cáncer de próstata Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Complutense University Associate Professor
Álvaro Taus Servicio Oncología Hospital del Mar 17 Mayo 2014
 Álvaro Taus Servicio Oncología Hospital del Mar 17 Mayo 2014 Introducción Epidemiología CPCNP Tratamientos dirigidos TERAPIAS ANTI-EGFR Erlotinib Gefitinib Afatinib Caso clínico TERAPIAS ANTI-ALK Crizotinib
Álvaro Taus Servicio Oncología Hospital del Mar 17 Mayo 2014 Introducción Epidemiología CPCNP Tratamientos dirigidos TERAPIAS ANTI-EGFR Erlotinib Gefitinib Afatinib Caso clínico TERAPIAS ANTI-ALK Crizotinib
Medicina individualizada: Cáncer de mama. Cáncer heredofamiliar. Encarna Adrover CHUA Albacete
 Medicina individualizada: Cáncer de mama. Cáncer heredofamiliar Encarna Adrover CHUA Albacete Bases terapéuticas del cáncer mama Radiología Clínica Comité multidisciplinar Tratamiento de la lesión Tratamiento
Medicina individualizada: Cáncer de mama. Cáncer heredofamiliar Encarna Adrover CHUA Albacete Bases terapéuticas del cáncer mama Radiología Clínica Comité multidisciplinar Tratamiento de la lesión Tratamiento
Experiencia con vinflunina en pacientes con cáncer urotelial e ILP prolongado
 Experiencia con vinflunina en pacientes con cáncer urotelial e ILP prolongado Cáncer urotelial estadio IV Estrategia de tratamiento en 2ª línea El tratamiento del carcinoma urotelial avanzado tras fracaso
Experiencia con vinflunina en pacientes con cáncer urotelial e ILP prolongado Cáncer urotelial estadio IV Estrategia de tratamiento en 2ª línea El tratamiento del carcinoma urotelial avanzado tras fracaso
ESTUDIO OBINDIAB GRUPO DE DIABETES SEMFYC
 ESTUDIO OBINDIAB GRUPO DE DIABETES SEMFYC METHODS CHARACTERISTICS OF THE PATIENTS Mean (SD) Range CI95% Age (years) 68,9+11,3 40-95 (67,8-70,0) HbA1c (%) 6,97+1,2 5,0-14,7 (6,9-7,1) Gender Male Female
ESTUDIO OBINDIAB GRUPO DE DIABETES SEMFYC METHODS CHARACTERISTICS OF THE PATIENTS Mean (SD) Range CI95% Age (years) 68,9+11,3 40-95 (67,8-70,0) HbA1c (%) 6,97+1,2 5,0-14,7 (6,9-7,1) Gender Male Female
Thank you. US English US Spanish. Australia-English Canada-English Ireland-English New Zealand-English Taiwan-English United Kingdom-English
 Dear Healthcare Provider, Included in this PDF are recruitment brochures in several languages to be used in MM Bone study (Protocol No.: 20090482). Kindly note these brochures have been updated according
Dear Healthcare Provider, Included in this PDF are recruitment brochures in several languages to be used in MM Bone study (Protocol No.: 20090482). Kindly note these brochures have been updated according
74 Prime Time. conjetura Suposición acerca de un patrón o relación, basada en observaciones.
 A abundant number A number for which the sum of all its proper factors is greater than the number itself. For example, 24 is an abundant number because its proper factors, 1, 2, 3, 4, 6, 8, and 12, add
A abundant number A number for which the sum of all its proper factors is greater than the number itself. For example, 24 is an abundant number because its proper factors, 1, 2, 3, 4, 6, 8, and 12, add
Aneurisma de aorta abdominal. Cirugía endovascular versus cirugía abierta? Dr Carlos Esteban Gracia. Germans Trias i Pujol Hospital. Badalona.
 Aneurisma de aorta abdominal Cirugía endovascular versus cirugía abierta? Dr Carlos Esteban Gracia. Germans Trias i Pujol Hospital. Badalona. En pacients amb aneurisma d aorta abdominal i amb risc quirúrgic
Aneurisma de aorta abdominal Cirugía endovascular versus cirugía abierta? Dr Carlos Esteban Gracia. Germans Trias i Pujol Hospital. Badalona. En pacients amb aneurisma d aorta abdominal i amb risc quirúrgic
Farmacogenética y Farmacogenómica. Su aplicación en la gestión clínica diaria.
 Farmacogenética y Farmacogenómica. Su aplicación en la gestión clínica diaria. Montserrat Baiget Servicio de Genética Hospital de la Santa Creu i Sant Pau Barcelona EMA (European Medicines Agency) Genomic
Farmacogenética y Farmacogenómica. Su aplicación en la gestión clínica diaria. Montserrat Baiget Servicio de Genética Hospital de la Santa Creu i Sant Pau Barcelona EMA (European Medicines Agency) Genomic
PANITUMUMAB EN CANCER DE COLON METASTÁSICO:
 PANITUMUMAB EN CANCER DE COLON METASTÁSICO: Romero Soria L 1, Jaraquemada Peláez T 2, Martin Clavo S 1, Rivero Cava MS 1, Braga Fuentes JL, Rangel Mayoral JF 1. 1 Servicio de Farmacia Hospitalaria 2 Servicio
PANITUMUMAB EN CANCER DE COLON METASTÁSICO: Romero Soria L 1, Jaraquemada Peláez T 2, Martin Clavo S 1, Rivero Cava MS 1, Braga Fuentes JL, Rangel Mayoral JF 1. 1 Servicio de Farmacia Hospitalaria 2 Servicio
Inhibición irreversible de EGFR: experiencia clínica en primera. EGFR mutado. Edurne Arriola Hospital del Mar Barcelona
 Inhibición irreversible de EGFR: experiencia clínica en primera línea de tratamiento de CPNCP EGFR mutado Edurne Arriola Hospital del Mar Barcelona Inhibición de EGFR Aproximadamente entre un 10 15% de
Inhibición irreversible de EGFR: experiencia clínica en primera línea de tratamiento de CPNCP EGFR mutado Edurne Arriola Hospital del Mar Barcelona Inhibición de EGFR Aproximadamente entre un 10 15% de
MANUAL DE FARMACIA CLINICA Y ATENCION FARMACEUTICA. EL PRECIO ES EN DOLARES BY JOAQUIN HERRERA CARRANZA
 MANUAL DE FARMACIA CLINICA Y ATENCION FARMACEUTICA. EL PRECIO ES EN DOLARES BY JOAQUIN HERRERA CARRANZA DOWNLOAD EBOOK : MANUAL DE FARMACIA CLINICA Y ATENCION HERRERA CARRANZA PDF Click link bellow and
MANUAL DE FARMACIA CLINICA Y ATENCION FARMACEUTICA. EL PRECIO ES EN DOLARES BY JOAQUIN HERRERA CARRANZA DOWNLOAD EBOOK : MANUAL DE FARMACIA CLINICA Y ATENCION HERRERA CARRANZA PDF Click link bellow and