Section One: Enrollment Inspection of Confidential Records Referral Record Change of Status Child Plus Application Form District Enrollment Forms
|
|
|
- José Ignacio Cano Segura
- hace 8 años
- Vistas:
Transcripción
1 HEAD START FORMS

2 Section One: Enrollment Inspection of Confidential Records Referral Record Change of Status Child Plus Application Form District Enrollment Forms Notification Letter (optional if prior to school starting) Parent Handbook/Student Handbook Code of Conduct Copy of Birth Certificate Copy of Social Security card Video Surveillance Policy (as needed) Legal Document Log
 Legal")
3 If you have reviewed all this student s Education Folder and do not find the information you are looking for, please ask a staff member.

4 Head Start INSPECTION OF CONFIDENTIAL RECORD NAME TITLE DATE PURPOSE

5 Head Start REFERRAL HEALTH/EDUCATION CHILD S NAME DATE TYPE OF REFERRAL REFERRAL CONTACT FOLLOW UP DATE COMMENTS INITIAL OF REFERRING STAFF

6 Head Start CHANGE OF STATUS Effective Date: Name of Child: Drop Re-enrollment Reason: Center: Teacher: Child withdraws before 10:00 a.m. /use that days date as drop date; Child withdraws after 10:00 a.m. /use the next days date as drop date Transfer Campus: Teacher: Reason: Change of Address: Change of Phone: Change of Employment: Mother Father Name: Place of Employment: Company: Phone: Person to Contact in case of Emergency: Name: Relationship: Phone: Submitted by: Title: Date: Mother or Dad s Signature: Date: 4/06

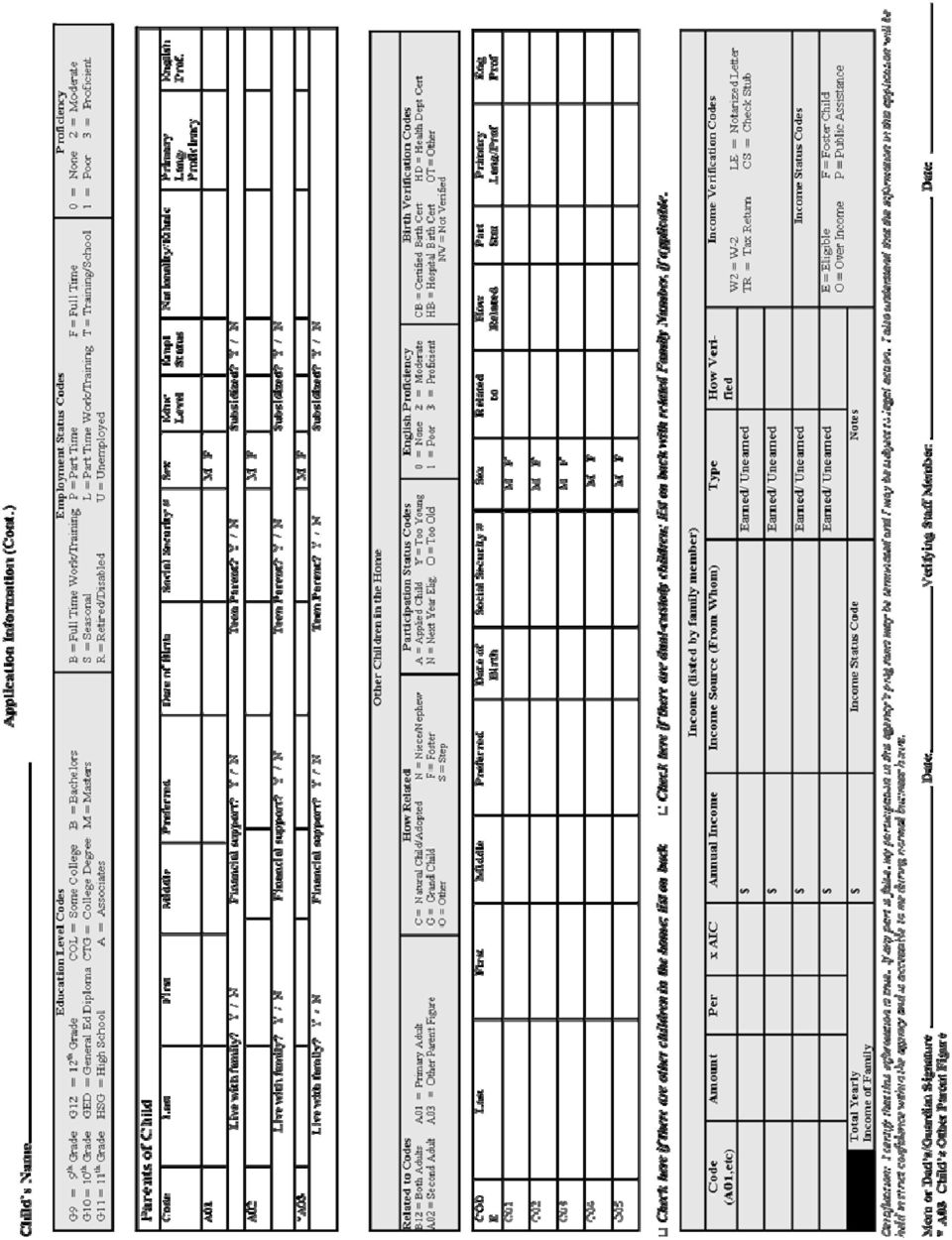
7 Applicant Information Complete for individuals who are applying to a program. Child s Information Last First Middle Preferred Birthday: SSN Gender: Male Female Place of Birth: Adult Name Child s Relationship Custody? Parental Status: One Two Yes No Number in Family Number in Household Yes No Primary Language At Home Number of Children By age: 0-3 By age: 4-5 Releases Signed? Yes No Date Signed TANF Status: YES NO SSI: YES NO WIC: YES NO Living Address Address/Phone Mailing Address Living Address Line 2 Mailing Address Line 2 City State Zip County City State Zip Phone Type if Primary Phone Number Phone Number Phone Note ( ) ( ) ( ) ( ) Medicaid Eligibility Status: On Medicaid Potentially Eligible Primary Health Coverage Other Health Coverage Health Coverage Not Eligible Medicaid Number Insurance Number Demographics Race (check ALL that apply): Asian Black Hispanic White Native American Pacific Islander Other: Language English if Primary Proficiency Nationality Ethnicity Certification: I certify that this information is true. If any part is false, my participation in this agency s programs may be terminated and I may be subject to legal action. I also understand that the information in this application will be held in strict confidence within the agency and is accessible to me during normal business hours. Mom or Dad s/guardian Signature Date Verifying Staff Member Date Page 1 of 2 Copyright 2004 Management Information Technology USA, Inc. 4/06

8
9 Informacion de Aplicante - Applicant Information Complete for individuals who are applying to a program. Información sobre su niño - Child s Information Apellido - Last Primer Nombre - First Segundo Nombre - Middle Nombre preferido - Preferred Fecha de Cumpleaños - Birthday: Número de Seguro Social - SSN Sexo - Gender: M F Ciudad, estado de nacimiento - Place of Birth: Nombre de Adulto Relación al Niño Adult Name Child s Relationship Date Signed Releases Signed? Yes No Es guardián? Custody? Si - Yes No - No Si - Yes No - No Cuántos padres viven en casa? Parental Status: Uno - One Dos - Two Cuántos en la familia? Number in family Cuántos viven en casa? Number in household Idioma que se habla en casa Primary Language At Home Cuántos niños en casa? Number of Children Por edad: 0-3 By age: 0-3 Por edad: 4-5 By age: 4-5 TANF Status: YES NO SSI: YES NO WIC: YES NO Dirección de casa - Living Address Dirección de Casa/ Número de Teléfono - Address/Phone Dirección de correo - Mailing Address Línea adicional para dirección de casa - Living Address Line 2 Línea adicional para dirección de correo - Mailing Address Line 2 Ciudad - City Estado - State Código Postal Zip Condado- County Ciudad - City Estado - State Código Postal Zip Tipo de teléfono Phone Type if Primary Número de Teléfono Phone Number Numero de Teléfono Phone Number Phone Note ( ) ( ) ( ) ( ) Medicaid Eligibility Status: On Medicaid Not Eligible Potentially Eligible Nombre de su seguro de salud - Primary Health Coverage Información sobre seguro de salud - Health Coverage Número de Medicaid - Medicaid Number Nombre de seguro de salud adicional - Other Health Coverage Número de su seguro de salud - Insurance Number Raza (favor de indicar todos lo que pertenecen) Race (check ALL that apply): Asiático - Asian Negro - Black Hispano - Hispanic Anglo - White Indio - Native American Indio de las islas Pacificas - Pacific Islander Otra raza - Other: Información Demográfica - Demographics Idioma - Language Ingles - English si es su idioma primaria if Primary Proficiency Nacionalidad - Nationality Su etnicidad - Ethnicity Certificación: Certifico que esta información es la verdad. Si alguna parte no es la verdad, mi participación en los programas de esta agencia pueden ser terminados y quizás resultará en acción legal. También entiendo que esta información está dada en confianza estricta dentro de esta agencia y tengo acceso de esta información durante las horas de negocio de esta agencia. Padre/Guardian Fecha Verifying Staff Member Date Copyright 2004 Management Information Technology USA, Inc. 4/06

10

11 NOTIFICATION LETTER Head Start Center: Address: Telephone: Date: Dear Parent/Guardian, Your HEAD START application for has been screened and the results are indicated by the check mark below: Your child has been approved for the Head Start program. Your child has been approved, but because our classes are presently filled, has been placed on our waiting list. Your child is too young for Head Start, this year. Your family income makes your child ineligible at this time. Your child s name will be considered for enrollment on this basis. If your child is accepted for enrollment at a later time, you will be notified. If your child has been approved, an enrollment time and place have been written in below. ENROLLMENT DATE LOCATION TIME Completion of enrollment will take between 1 and 1 ½ hours. Please bring your Medicaid card and a copy of current physical and dental records, if you have one, and proof of any insurance you may have. Sincerely, Head Start Representative 4/06

12 CARTA DE NOTIFICACION Head Start Escuela: Dirección: Número de Teléfono: Fecha: Estimados Padres/Guardianes, Su aplicación en el programa de HEAD START para ha sido revisada y el resultado está marcado: (Nombre del niño) Su hijo ha sido aprobado para el programa de Head Start. Su hijo ha sido aprobado pero porque nuestras clases ya tienen el límite de niños, hemos puesto el nombre de su niño en una lista de espera. Su hijo está muy joven para el programa de Head Start este año. El salario de su familia hace que su niño sea inelegible horita. Su niño no será considerado por esta razón. Si aceptamos a su hijo en el futuro, le notificaremos. Si hemos aceptado a su niño, la fecha, el tiempo de matriculación y el lugar en donde recibirse está escrito abajo. FECHA DE MATRICULACION HORA LUGAR/ESCUELA Se tomará aproximadamente una hora en matricular a su hijo. Favor de traer su tarjeta de Medicad, si lo tiene, o prueba de seguro. Sinceramente, Representante de Head Start 5/2007

13 OPTIONAL ENROLLMENT FORMS Thank You Letter for Your Interest Video Surveillance Policy

14 Dear Parent/Guardian: Head Start Thank you for your interest in our Head Start Child Development Program. To be considered for the program, we must have reasonable verification of 12 months income for your total family. Examples of this verification could be: A copy of your current income tax (please note this is a federally sponsored program) OR W-2 forms for parents or guardians Income earned in previous 12 months (notarized family statement of gross earnings, 12 months worth of check stubs). Eligibility might be able to be determined with lesser documentation, but that will slow the eligibility process. Also, please understand that we will need to determine your family composition for eligibility, i.e. total in household including children. You will need to bring documentation of any additional non-taxable income you receive: Child Support Social Security Benefits Unemployment Compensation Dividends, Interest Welfare Payments Pensions, Annuities Workers Compensation Alimony Educational Loans/Grants Other necessary documentation to bring is your child s: Birth Certificate Social Security Card Shot Record Food Stamp Letter TANF Documentation Proof of medical and/or dental insurance When you come in to bring the information requested, it will take 15 to 30 minutes to complete the eligibility form. If you have any questions, please feel free to call our office at. Thank you for your cooperation. 5/2007
. Eligibility might be able to be determined with lesser documentation, but that will slow the eligibility process.")
15 Estimado Padre/Guardián, Head Start Muchas gracias por su interés en el programa de Desarrollo de Niños de Head Start. Para ser considerado en el programa, tenemos que recibir 12 meses de verificación de salario de su familia en total. Ejemplos de verificación pueden ser: Copia de su declaración de impuestos federales, O Formas de W-2 de los padres/guardianes, Los recibos (de 12 meses) de sueldo. Podemos determinar elegibilidad con menos documentación, pero el proceso tomará más tiempo. También, favor de entender que necesitaremos determinar su elegibilidad considerando todas personas en su familia, incluyendo los niños. Necesitará traer documentación de ingresos adicionales que recibe. Por ejemplo: Sostén de niño (resultado de divorcio) Beneficios de Seguro Social Beneficios de desocupación Dividendo, Interés (de dinero) Pagos de ayuda del Estado (para su bienestar) Pensión, anualidad Compensación de trabajo Asistencia (resultado de divorcio) Préstamos educacionales/donaciones Otros documentos de su hijo que son necesario traer: Certificado de nacimiento Tarjeta de seguro social Forma/record de inmunizaciones Carta del estado acerca de poder recibir estampillas para comida TANF un programa del gobierno de Texas para familias en necesidad de ayuda Prueba de seguro médico o dental Cuando usted venga a traer la información requerida, tomará 15 a 30 minutos para completar la forma de elegibilidad. Si usted tiene cualquier pregunta, favor de llamar nuestra oficina. Muchas gracias por su cooperación.

16 Video Surveillance Policy Head Start Dear Parents, This is to notify you of our classroom video surveillance cameras. The purpose of the video cameras is for your child s safety as well as the Head Start center teachers, staff and parents. We take pride in providing the best childcare and learning environment, our preventative measure is to video tape your children in their classrooms. Head Start has posted video surveillance signs in the classrooms and around the Head Start building to inform the general public of the Head Start video cameras. Extreme care is enforced in safeguarding these surveillance tapes against unauthorized use. After reading the above notice, I Head Start classroom. the parent/legal guardian of understand that my children will be under videotape surveillance while in the I understand that the surveillance cameras in the classrooms are there to protect the welfare of my children, and the Head Start staff and teachers. Parent/Guardian Date Site Manager Date 4/04

17 PÓLIZA DE VIGILANCIA DE VIDEO Head Start Estimados Padres, Esta carta es para notificarle de nuestras cámaras de video para vigilancia en los salones de clase. El propósito de las cámaras de video es para la seguridad de su niño así como la seguridad de las maestras de Head Start, los empleados de Head Start, y los padres de los niños. Tomamos mucho orgullo en proveer el mejor cuidado de su niño y ambiente de aprender. Nuestro método preventivo es de tomar video durante el tiempo que los niños están en sus clases. Head Start ha puesto rótulos dentro de y alrededor de la escuela que anuncian al público de las cámaras de video para vigilancia. Tomamos cuidado en la salvaguardia de estos videos contra abuso ilegal. Después de leer esta carta, yo el padre/guardián legal de entiendo que mis niños estarán bajo vigilancia de cámaras de video durante su tiempo en el programa de Head Start. Entiendo que las cámaras de vigilancia en las clases están allí para proteger el bienestar de mis niños y los empleados de Head Start. Padre/Guardián Fecha Empleado de Head Start Fecha

18 INCOME DOCUMENTATION Eligibility Worksheet Individual Systematic Form Committee Systematic Form Signature Page Group Systematic Selection Form

19 ELIGIBILITY Family Size (total # in household) Family s Gross Annual Income (parents only) ITEM $ $ A) Taxable income earned (computed in the following ways) 1) Income earned in previous calendar year (from Federal Income Tax Form) 2) Income earned in previous 12 months (family statement of gross earnings) $ $ (B) Additional non-taxable income 1) Veteran s benefits $ 2) Social Security benefits $ 3) Unemployment compensation $ 4) Dividends, interest $ 5) Welfare payments $ 6) Pensions, annuities $ 7) Workers Compensation $ 8) Alimony $ 9) Child Support $ 10) Educational loans/grants $ C) Total of B $ D) Total of A & B $ E) Deductions (medical & dental expenses and casualty or theft loss in excess of 10% of gross family income) $ F) Total (adjusted gross family income = E minus D) $ MAXIMUM ALLOWABLE INCOME FOR FAMILY SIZE $ ABOVE INCOME $ BELOW INCOME $ I (we) agree to report any and all changes as they occur in my (our) family s income during the period my (our) children are enrolled in the program. I also understand that I am required to furnish written proof of all income information on this form. I hereby affirm that all the information given above is accurate. Date Verifier s Signature Mom or Dad/Guardian s Signature 5/2007
 Total of B $ D) Total of A & B $ E) Deductions (medical & dental expenses and casualty or theft loss in excess of 10% of gross family income) $ F) Total (adjusted gross family")
20 File in confidential folder for income Region 9 Head Start Individual Systematic Selection Form Head Start This information is to be used with professional staff only in keeping with FERPA and I.D.E.A. B Confidentiality Requirements and Head Start performance Standards. Revised 4/2007

21 File in ERSEA Binder Region 9 Head Start Committee Systematic Selection Form Signature Page ISD Head Start (a) Approved Over Income Birth Date Child Age as of Sept. 1 Code # # in Family Male/Female Single Parent Home Disabilities Family Income Below Poverty Guideline on Public Assistance Child in Foster Care Non Parent Guardian Family Preservation/Open CPS Case Family is on TANF Family is Homeless Child has Obvious Medical Need Stressors (See Application Checklist) Early Head Start Transfer/ Even Start Child is Non English Speaking Family has 3 or more Children Parent Employment or Training Totals Date of Application 15 20/10/ pts. each /10 Signature of Systematic Selection Date Committee Member Date This information is to be used with professional staff only in keeping with FERPA and I.D.E.A. B confidentiality requirements and Head Start performance Standards. Revised 8/2007
22 File in ERSEA Binder ISD Region 9 Head Start Group Systematic Selection Form Signature Page Head Start (a) Approved Over Income Birth Date Child Age as of Sept. 1 Code # # in Family Male/Female Single Parent Home Disabilities Family Income Below Poverty Guideline on Public Assistance Child in Foster Care Non Parent Guardian Family Preservation/Open CPS Case Family is on TANF Family is Homeless Child has Obvious Medical Need Stressors (See Application Checklist) Early Head Start Transfer/ Even Start Child is Non English Speaking Family has 3 or more Children Parent Employment or Training Totals Date of Application 15 20/10/ pts. each /10 This information is to be used with professional staff only in keeping with FERPA and I.D.E.A. B confidentiality requirements and Head Start performance Standards. Revised 8/2007
23 APPLICATION CHECKLIST
24 Head Start Child s Name: APPLICATION CHECKLIST POINT SYSTEM: Stressors (2 points each) Lack of transportation..family does not have private vehicle Child living with relatives Explain: CPS Intervention investigation Family living with relatives Education level below 12 th grade Teenage Parent (when Head Start child was born - between 13-19) Migrant Family.family has moved several times in the past 12 mos. seasonal/agricultural work Parent Deployed Parent Disability Sibling Disability Pregnancy Recent Relocation.within 6 months Recent Unemployment.within 6 months Working and in school (including GED classes, Vo Tech, College) Other Explain: Disability (5, 10 or 20 points) Suspected ECI (Early Childhood Intervention) or other program for children with disabilities Qualified for special education services Medical (10 points) Child has obvious medical need Transition/Transfers (15 points) Even Start Project Together/Early Head Start Transfer (from another Head Start Program) Other Homeless (20 points) please explain: Non-parent Guardian (100 points) Family Preservation (30 points) Parent Employment or Training (20 points) both or (10 parents) one MUST HAVE: Child s: Birth Certificate Social Security Card Medicaid/Insurance Card Shot Record Parent s: Proof of Income Picture I.D. PLEASE ASK ABOUT THE FOLLOWING: (Check if attached, if not checked, explain status) Physical exam Status: Dental exam Status: Approved Verified by:
25 Section Two: Health Consent for Health Services Emergency Consent and Medical Information Release Form Copy of Health Contact Follow-up Form (as needed) Documentation of Insurance (Medicaid/Chips, etc.) Child Health-Form 2A,6 Head Start Health Services Release of Information Child Health Form 3 - Physical Hearing and Vision for 3 year old Copy of Immunization Record Lead Screening/TB screening Child Health Record Form 5 - Dental Child Plus Growth Charts Head Start Observation Notes In House Referral (as needed) Accident Report (as needed)
26 Head Start Consent for Health Services I, hereby give my consent for the child listed below to receive the screening tests and examinations checked below, and for transport of the child to and from the services as needed. I understand these services are deemed necessary or advisable by the Head Start program and that I will be informed of any results that are not normal. I also understand that is my responsibility to provide Head Start with an up-to-date immunization record and a record of medical and dental examinations performed in the past year. This consent is valid for one year after the signed date. The purpose of this consent has been explained to me. I agree: That in case of emergency or if a parent or guardian cannot be contacted, Head Start may provide first aide or emergency medical care if needed. Yes No Initial below: Developmental Screening Medical Examination Speech Screening Hearing Test Immunizations (if necessary) Mental Health Screening Crisis Counseling Dental Examination Height and Weight Vision Test T.B. Test Brush teeth daily with fluoride toothpaste Lead Screening I understand that this involves a blood sample obtained by a fingerstick or venipuncture if necessary. As a parent/guardian of, I hereby authorize the release of Medicaid/THSTEPS eligibility information and medical records to satisfy Head Start requirements. CHILD S NAME DATE OF BIRTH Signature of Mom or Dad/Guardian Relationship to Child Date I have explained to the purpose of this release and the nature of the tests and examinations that the children enrolled in Head Start receive. Signature of Head Start Staff Date
27 PERMISO PARA RECIBIR SERVICIOS DE SALUD Head Start Yo, doy permiso que mi hijo obtenga los exámenes que he designado en la siguiente parte de esta forma. Además, doy permiso que alguien del programa de Head Start lo transporte para recibir estos servicios. Entiendo que mi hijo necesita estos exámenes y que me avisarán si un examen no resulte en manera normal. También entiendo que es mi responsabilidad proveerle a Head Start con los record corrientes de inmunizaciones de mi hijo y examen hechos por un médico o dentista dentro del año pasado. Esta forma está en efecto por un año desde hoy. Me han explicado el propósito de esta forma. Estoy en acuerdo: Que si hay alguna emergencia en donde no me pueden comunicar por teléfono, el personal de Head Start puede proveer auxilio de emergencia si es necesario. Si No Favor de marcar los servicios que necesita su hijo: Examen de desarrollo Examen de salud mental Examen por un medico Examen por consejero de crisis Examen por un dentista Examen para manera de habla Examen para saber que tan alto está y cuanto pesa mi hijo Examen auditiva Examen de visión Inmunizaciones (si es necesario) Examen para tuberculosis Examen para ver si se cepilla los dientes con pasta de diente que contiene fluoruro Examen que indica si el niño se ha puesto en contacto con plomo. (En años pasados los cuartos en casas eran pintados con pintura que tenía plomo. Este plomo es como veneno si uno se pone en contacto con el.) En este examen se le tiene que obtener sangre por un dedo. Como padre/guardián de, yo doy permiso que el programa/personal de Head Start puedan usar la información de Medicad/THSTEPS y los record médicos de mi hijo. NOMBRE DE NIÑO FECHA DE NACIMIENTO Firma de padre/guardián Parentesco al niño Le he explicado a niños de Head Start. Firma de personal de Head Start Fecha el propósito de esta forma y los servicios de salud que reciben los Fecha
28 Head Start Emergency Consent and Medical Information Release Form Name of Child: Birth Date: Sex: Address: Student Social Security : School: Teacher: In the event that I cannot be reached to make arrangements for medical attention for my child, at the time of an accident or illness while he or she is attending a Head Start program, I grant and authorize a representative of Head Start to grant permission to the medical staff and the Emergency Department staff of the local hospital to perform any medical or surgical treatment and to administer such anesthesia and/or drugs as may be deemed necessary in the diagnosis or treatment of said patient. Furthermore, I hereby authorize release of all medical/dental pertinent information concerning my child to a designated representative of Head Start. We the parent(s)/guardian(s) of the above named child acknowledge it is our responsibility to keep the information in this Emergency Consent form current and correct. We agree to notify Head Start of any changes to phone numbers or changes of physician or changes in name of those who shall be contacted in the event of any emergency. Medications Taken By Child: Child s Allergies: Chronic Diseases: Child s Doctor: Child s Dentist: Signature of Mom or Dad Date Home Phone Work Phone 4/06
29 Permiso Para Divulgar Información de Emergencia y Medico Head Start Nombre del niño: Fecha de nacimiento: Sexo: Su dirección: Número de seguro social (del niño): Nombre de escuela: Nombre de su maestra: Durante el tiempo que mi niño esté bajo el cuidado del programa de Head Start, doy permiso que los empleados de Head Start arreglen que mi niño tenga tratamiento de emergencia si es que no se puedan ponerse en contacto conmigo. Les doy permiso a los empleados de Head Start que autoricen al Departamento de Emergencia que le den a mi hijo anestesia y/o drogas que sean necesarias para el bienestar de mi hijo. Además, doy permiso al personal de Head Start que puedan divulgar información de mi hijo acerca de su salud física o dental a personal de Head Start. Nosotros, los padres/guardianes de este niño reconocemos que es nuestra responsabilidad de asegurar que esta forma tenga la más reciente información acerca de la salud de mi niño y los nombres y números de teléfono de emergencia. Aseguramos decirles a los empleados de Head Start cuando haya cambio de médico y su número de teléfono o los nombres y números de teléfono de la gente a quien se le puede llamar en caso de emergencia. Nombres de las medicinas que toma mi hijo: Alergias que tiene mi hijo: Enfermedades crónicas: El nombre de su doctor: El nombre de su dentista: / Firma de mamá o papá/guardián Fecha: Número de teléfono de casa/trabajo
30 Head Start Health Contact Follow-up Form This is a summary for the child listed below. We hope that it will be of assistance to you. Child s name Date Screening completed Results were normal Yes/No Date of Followup/Treatment Results Hearing Vision Dental Additional Information: Staff Signature/Date File in Health Section and Give copy to Parent 4/06
31 Forma de Continuación De Información de Salud Head Start Esta forma sirve como sumario de examines para el niño cuyo nombre sigue. Esperamos que le ayude. Nombre del niño Examen de oídos Fecha que se cumplió el examen Los resultados son normales Si/No Fecha para continuación de tratamiento Los resultados Examen de visión Examen dental Información adicional: Firma de Personal/Fecha File in Health Section and Give copy to Parent
32 CHILD HEALTH RECORD: FORM 2A, HEALTH HISTORY TO BE COMPLETED BY HEAD START STAFF DURING PARENT/GUARDIAN INTERVIEW. HEAD START CENTER: CHILD S NAME: SEX: BIRTHDATE: PERSON INTERVIEWED: DATE: RELATIONSHIP: NAME OF INTERVIEWER: TITLE: PREGNANCY/BIRTH HISTORY YES NO EXPLAIN YES ANSWERS 1. DID MOTHER HAVE ANY HEALTH PROBLEMS DURING THIS PREGNANCY OR DURING DELIVERY? 2. DID MOTHER VISIT PHYSICIAN FEWER THAN TWO TIMES DURING PREGNANCY? 3. WAS CHILD BORN OUTSIDE OF A HOSPITAL? 4. WAS CHILD BORN MORE THAN 3 WEEKS EARLY OR LATE? 5. WHAT WAS CHILD S BIRTH WEIGHT? lbs., oz. 6. WAS ANYTHING WRONG WITH CHILD AT BIRTH? 7. WAS ANYTHING WRONG WITH CHILD IN THE NURSERY? 8. DID CHILD OR MOTHER STAY IN HOSPITAL FOR MEDICAL REASONS LONGER THAN USUAL? 9. IS MOTHER PREGNANT NOW? (If yes, ask about prenatal care, or schedule time to discuss prenatal care arrangements.) HOSPITALIZATIONS AND ILLNESSES YES NO EXPLAIN YES ANSWERS 10. HAS CHILD EVER BEEN HOSPITALIZED OR OPERATED ON? 11. HAS CHILD EVER HAD A SERIOUS ACCIDENT (broken bones, head injuries, falls, burns, poisoning)? 12. HAS CHILD EVER HAD A SERIOUS ILLNESS? HEALTH PROBLEMS YES NO EXPLAIN (Use additional sheets if needed) 13. DOES CHILD HAVE FREQUENT SORE THROAT; Cough; URINARY INFECTIONS OR TROUBLE URINATING; STOMACH PAIN, VOMITING, DIARRHEA? 14. DOES CHILD HAVE DIFFICULTY SEEING (Squint, cross eyes, look closely at books)? * 15. IS CHILD WEARING (Or supposed to wear) GLASSES? 16. DOES CHILD HAVE PROBLEMS WITH EARS/HEARING (Pain in ear, frequent earaches, discharge, rubbing or favoring one ear)? 17. HAVE YOU EVER NOTICED CHILD SCRATCHING HIS/HER BEHIND (Rear end, anus, butt) WHILE ASLEEP? 18. HAS CHILD EVER HAD A CONVULSION OR SEIZURE? IS CHILD TAKING MEDICINE FOR SEIZURES 19. IS CHILD TAKING ANY OTHER MEDICINE NOW? (Special consent form must be signed for Head Start to administer any medication). 20. IS CHILD NOW BEING TREATED BY A PHYSICIAN OR A DENTIST? 21. HAS CHILD HAD: BOILS, CHICKENPOX, ECZEMA, GERMAN MEASLES, MEASLES, MUMPS, SCARLET FEVER, WHOOPING COUGH? 22. HAS CHILD HAD: HIVES, POLIO? * 23. HAS CHILD HAD: ASTHMA, BLEEDING TENDENCIES DIABETES, EPILEPSY, HEART/BLOOD VESSEL * DISEASE, LIVER DISEASE, RHEUMATIC FEVER, SICKLE CELL DISEASE? 24. DOES CHILD HAVE ALLERGY PROBLEMS (Rash, itch swelling, difficulty breathing, sneezing)? a. WHEN EATING ANY FOODS? * b. WHEN TAKING ANY MEDICATION? c. WHEN NEAR ANIMALS, FURS, INSECTS, DUST, ETC? 25. (If any yes answers to questions 14, 16, 18, 22, 23, or 24 ask:) DO ANY OF THE CONDITIONS WE VE TALKED ABOUT SO FAR GET IN THE WAY OF THE CHILD S EVERYDAY ACTIVITIES? * * (If yes ) WAS LAST CHECKUP MORE THAN ONE YEAR AGO? If yes, ask WHEN DID IT LAST HAPPEN? WHAT MEDICINE? WHAT MEDICINE? (If yes ) WILL IT NEED TO BE GIVEN WHILE CHILD IS AT HEAD START? HOW OFTEN? (PHYSICIAN S NAME: ) If yes, transfer information to Forms 1 & 5. If yes, TRANSFER INFORMATION TO Forms 1 & 5. WHAT FOODS? WHAT MEDICINE? WHAT THINGS? HOW DOES CHILD REACT? DESCRIBE HOW: DID A DOCTOR OR OTHER HEALTH PROFESSIONAL TELL YOU THE CHILD HAS THIS PROBLEM? WHEN? 26. ARE THERE ANY CONDITIONS WE HAVEN T TALKED ABOUT DESCRIBE HOW: THAT COULD GET IN THE WAY OF THE CHILD S EVERYDAY ACTIVITIES? DID A DOCTOR OR OTHER HEALTH PROFESSIONAL TELL YOU THE CHILD HAS THIS PROBLEM? WHEN? * If starred (*) questions have yes answers, go to question 25. 4/06
33 CHILD HEALTH RECORD: FORM 2A, HEALTH HISTORY (Continued) PERSON INTERVIEWED: DATE: RELATIONSHIP: NAME OF INTERVIEWER: TITLE: PHYSICAL, PSYCHOLOGICAL, AND SOCIAL DEVELOPMENT THESE QUESTIONS WILL HELP US UNDERSTAND YOUR CHILD BETTER AND KNOW WHAT IS USUAL FOR HIM/HER AND WHAT MIGHT NOT BE USUAL THAT WE SHOULD BE CONCERNED ABOUT: 27. CAN YOU TELL ME ONE OR TWO THINGS YOUR CHILD IS INTERESTED IN OR DOES ESPECIALLY WELL? 28. DOES YOUR CHILD TAKE A NAP? NO, YES. IF YES DESCRIBE WHEN AND HOW LONG. 29. DOES YOUR CHILD SLEEP LESS THAN 8 HOURS A DAY OR HAVE TROUBLE SLEEPING (SUCH AS BEING FRETFUL, HAVING NIGHTMARES, WANTING TO STAY UP LATE)? NO, YES. IF YES DESCRIBE ARRANGEMENTS (OWN ROOM, OWN BED, AND SO FORTH). 30. HOW DOES YOUR CHILD TELL YOU HE/SHE HAS TO GO TO THE TOILET? 31. DOES YOUR CHILD NEED HELP IN GOING TO THE TOILET DURING THE DAY OR NIGHT, OR DOES YOUR CHILD WET HIS/HER PANTS? NO, YES. IF YES DESCRIBE. 32. HOW DOES YOUR CHILD ACT WITH ADULTS THAT HE/SHE DOESN T KNOW? 33. HOW DOES YOUR CHILD ACT WITH A FEW CHILDREN HIS/HER OWN AGE? 34. HOW DOES YOUR CHILD ACT WHEN PLAYING WITH A GROUP OF OTHER CHILDREN? 35. DOES YOUR CHILD WORRY A LOT, OR IS HE/SHE VERY AFRAID OF ANYTHING? NO, YES. IF YES, WHAT THINGS SEEM TO CAUSE HIM OR HER TO WORRY OR TO BE AFRAID? 36. CHILDREN LEARN TO DO THINGS AT DIFFERENT AGES. WE NEED TO KNOW WHAT EACH CHILD ALREADY CAN DO OR IS LEARNING TO DO EASILY AND WHERE THEY MIGHT BE SLOW OR NEED HELP SO WE CAN FIT OUR PROGRAM TO EACH CHILD. I M GOING TO LIST SOME THINGS CHILDREN LEARN TO DO AT DIFFERENT AGES AND ASK WHEN YOUR CHILD STARTED TO DO THEM, AS BEST YOU CAN REMEMBER. (INTERVIEWER: Read question for each item listed below, and check off the parent s answer in the appropriate space). EARLIER WHEN LATER AGE EXPECTED a. WOULD YOU SAY YOUR CHILD BEGAN TO EARLIER THAN YOU EXPECTED, ABOUT WHEN YOU EXPECTED, OR LATER THAN YOU EXPECTED? b. WHEN DID HE/SHE BEGIN TO? (a) SIT UP WITHOUT HELP (b) CRAWL (c) WALK (d) TALK (e) FEED AND DRESS SELF (f) LEARN TO USE THE TOILET (g) RESPOND TO DIRECTIONS (h) PLAY WITH TOYS (i) USE CRAYONS (j) UNDERSTAND WHAT IS SAID TO HIM/HER 37. DOES YOUR CHILD HAVE ANY DIFFICULTIES SAYING WHAT HE/SHE WANTS TO DO OR DO YOU HAVE ANY TROUBLE UNDERSTANDING YOUR CHILD? NO, YES. IF YES PLEASE DESCRIBE. 38. CHILDREN SOMETIMES GET CRANKY OR CRY WHEN THEY RE TIRED, HUNGRY, SICK, AND SO FORTH. DOES YOUR CHILD OFTEN GET CRANKY OR CRY AT OTHER TIMES, WHEN YOU CAN T FIGURE OUT WHY? NO, YES. IF YES CAN YOU TELL ME ABOUT THAT? WHEN THIS HAPPENS, WHAT DO YOU DO ABOUT IT TO HELP THE CHILD FEEL BETTER? 39. HAVE THERE BEEN ANY BIG CHANGES IN YOUR CHILD S LKIFE IN THE LAST SIX MONTHS? NO, YES. IF YES PLEASE DESCRIBE. 40. ARE YOU OR YOUR FAMILY HAVING ANY PROBLEMS NOW THAT MIGHT AFFECT YOUR CHILD? NO, YES. IF YES PLEASE DESCRIBE. 41. IS THERE ANYTHING ELSE YOU WOULD LIKE US TO KNOW ABOUT YOUR CHILD? NO, YES. IF YES PLEASE DESCIBE. 4/06
www.deltadentalins.com/language_survey.html
 Survey Code: Survey 1 February 6, 2008 Dear Delta Dental Enrollee: Recent changes in California law will require that all health care plans provide language assistance to their plan enrollees beginning
Survey Code: Survey 1 February 6, 2008 Dear Delta Dental Enrollee: Recent changes in California law will require that all health care plans provide language assistance to their plan enrollees beginning
Daly Elementary. Family Back to School Questionnaire
 Daly Elementary Family Back to School Questionnaire Dear Parent(s)/Guardian(s), As I stated in the welcome letter you received before the beginning of the school year, I would be sending a questionnaire
Daly Elementary Family Back to School Questionnaire Dear Parent(s)/Guardian(s), As I stated in the welcome letter you received before the beginning of the school year, I would be sending a questionnaire
El Abecedario Financiero
 El Abecedario Financiero Unidad 4 National PASS Center 2013 Lección 5 Préstamos Vocabulario: préstamo riesgocrediticio interés obligadosolidario A lgunavezpidesdineroprestado? Dóndepuedespedirdinero prestado?
El Abecedario Financiero Unidad 4 National PASS Center 2013 Lección 5 Préstamos Vocabulario: préstamo riesgocrediticio interés obligadosolidario A lgunavezpidesdineroprestado? Dóndepuedespedirdinero prestado?
HABERSHAM COUNTY SCHOOLS LAS ESCUELAS DEL CONDADO DE HABERSHAM ENROLLMENT/STUDENT INFORMATION FORM FORMA DE MATRICULACION
 HABERSHAM COUNTY SCHOOLS LAS ESCUELAS DEL CONDADO DE HABERSHAM ENROLLMENT/STUDENT INFORMATION FORM FORMA DE MATRICULACION CHILD LIVES IN SCHOOL DISTRICT (PLEASE GIVE NAME OF ELEMENTARY SCHOOL) (distrito
HABERSHAM COUNTY SCHOOLS LAS ESCUELAS DEL CONDADO DE HABERSHAM ENROLLMENT/STUDENT INFORMATION FORM FORMA DE MATRICULACION CHILD LIVES IN SCHOOL DISTRICT (PLEASE GIVE NAME OF ELEMENTARY SCHOOL) (distrito
TITLE VI COMPLAINT FORM
 [CITY SEAL/EMBLEM] The Capital City of the Palm Beaches TITLE VI COMPLAINT FORM Title VI of the 1964 Civil Rights Act requires that "No person in the United States shall, on the ground of race, color or
[CITY SEAL/EMBLEM] The Capital City of the Palm Beaches TITLE VI COMPLAINT FORM Title VI of the 1964 Civil Rights Act requires that "No person in the United States shall, on the ground of race, color or
TOUCH MATH. Students will only use Touch Math on math facts that are not memorized.
 TOUCH MATH What is it and why is my child learning this? Memorizing math facts is an important skill for students to learn. Some students have difficulty memorizing these facts, even though they are doing
TOUCH MATH What is it and why is my child learning this? Memorizing math facts is an important skill for students to learn. Some students have difficulty memorizing these facts, even though they are doing
Vision and Hearing Program Consent for Services. I, the parent/legal guardian of, give consent Please print name of child
 Vision and Hearing Program Consent for Services I, the parent/legal guardian of, give consent Please print name of child for the Cook County Department of Public Health to provide vision and/or hearing
Vision and Hearing Program Consent for Services I, the parent/legal guardian of, give consent Please print name of child for the Cook County Department of Public Health to provide vision and/or hearing
As the 2013-14 school year comes to a close, Camden City School District is excited to get summer programming underway!
 June 2014 Dear Parents and Guardians: As the 2013-14 school year comes to a close, Camden City School District is excited to get summer programming underway! The District Summer School Program will operate
June 2014 Dear Parents and Guardians: As the 2013-14 school year comes to a close, Camden City School District is excited to get summer programming underway! The District Summer School Program will operate
HEAD START MEDICATION ADMINISTRATION
 HEAD START MEDICATION ADMINISTRATION Dear Parents/Guardians: It is the policy of Head Start to cooperate with each Head Start child's parent/guardian and his/her physician by administering and providing
HEAD START MEDICATION ADMINISTRATION Dear Parents/Guardians: It is the policy of Head Start to cooperate with each Head Start child's parent/guardian and his/her physician by administering and providing
Down Payment Assistance Application Packet
 Down Payment Assistance Application Packet Please assure that all needed items are attached and complete. Please note that your application will not be considered until all documents are received. 1. Down
Down Payment Assistance Application Packet Please assure that all needed items are attached and complete. Please note that your application will not be considered until all documents are received. 1. Down
Child Care Assistance Program Búsqueda de Trabajo
 Child Care Assistance Program Búsqueda de Trabajo Usted ha pedido cuidado para sus niños mientras busca trabajo a través del programa de CCAP. Este programa ofrece un total de 30 días mientras busca trabajo.
Child Care Assistance Program Búsqueda de Trabajo Usted ha pedido cuidado para sus niños mientras busca trabajo a través del programa de CCAP. Este programa ofrece un total de 30 días mientras busca trabajo.
Learning Masters. Early: Force and Motion
 Learning Masters Early: Force and Motion WhatILearned What important things did you learn in this theme? I learned that I learned that I learned that 22 Force and Motion Learning Masters How I Learned
Learning Masters Early: Force and Motion WhatILearned What important things did you learn in this theme? I learned that I learned that I learned that 22 Force and Motion Learning Masters How I Learned
IRS DATA RETRIEVAL NOTIFICATION DEPENDENT STUDENT ESTIMATOR
 IRS DATA RETRIEVAL NOTIFICATION DEPENDENT STUDENT ESTIMATOR Subject: Important Updates Needed for Your FAFSA Dear [Applicant], When you completed your 2012-2013 Free Application for Federal Student Aid
IRS DATA RETRIEVAL NOTIFICATION DEPENDENT STUDENT ESTIMATOR Subject: Important Updates Needed for Your FAFSA Dear [Applicant], When you completed your 2012-2013 Free Application for Federal Student Aid
Students Pledge: Parents Pledge:
 The school-home compact is a written agreement between administrators, teachers, parents, and students. It is a document that clarifies what families and schools can do to help children reach high academic
The school-home compact is a written agreement between administrators, teachers, parents, and students. It is a document that clarifies what families and schools can do to help children reach high academic
2015 16 Student Eligibility Verification Advanced Placement/International Baccalaureate Test Fee Program
 2015 16 Student Eligibility Verification Advanced Placement (AP) and/or International Baccalaureate (IB) Exams AP Exam IB Exam AP and IB Exams I. Student Information Last Name First Name MI Grade High
2015 16 Student Eligibility Verification Advanced Placement (AP) and/or International Baccalaureate (IB) Exams AP Exam IB Exam AP and IB Exams I. Student Information Last Name First Name MI Grade High
Lump Sum Final Check Contribution to Deferred Compensation
 Memo To: ERF Members The Employees Retirement Fund has been asked by Deferred Compensation to provide everyone that has signed up to retire with the attached information. Please read the information from
Memo To: ERF Members The Employees Retirement Fund has been asked by Deferred Compensation to provide everyone that has signed up to retire with the attached information. Please read the information from
TITLE VI COMPLAINT FORM
 TITLE VI COMPLAINT FORM Before filling out this form, please read the Arcata and Mad River Transit System Title VI Complaint Procedures located on our website or by visiting our office. The following information
TITLE VI COMPLAINT FORM Before filling out this form, please read the Arcata and Mad River Transit System Title VI Complaint Procedures located on our website or by visiting our office. The following information
PRINTING INSTRUCTIONS
 PRINTING INSTRUCTIONS 1. Print the Petition form on 8½ X 11inch paper. 2. The second page (instructions for circulator) must be copied on the reverse side of the petition Instructions to print the PDF
PRINTING INSTRUCTIONS 1. Print the Petition form on 8½ X 11inch paper. 2. The second page (instructions for circulator) must be copied on the reverse side of the petition Instructions to print the PDF
2014 15 Student Eligibility Verification Advanced Placement/International Baccalaureate Test Fee Program
 2014 15 Student Eligibility Verification Advanced Placement (AP) and/or International Baccalaureate (IB) Exams þ AP Exam IB Exam AP and IB Exams I. Student Information Last Name First Name MI Grade High
2014 15 Student Eligibility Verification Advanced Placement (AP) and/or International Baccalaureate (IB) Exams þ AP Exam IB Exam AP and IB Exams I. Student Information Last Name First Name MI Grade High
What is family health history?
 Family Health History Project Pre-Survey What is family health history? Family health history is information about diseases that run in your family, as well as the eating habits, activities, and environments
Family Health History Project Pre-Survey What is family health history? Family health history is information about diseases that run in your family, as well as the eating habits, activities, and environments
Vermont Mini-Lessons: Leaving A Voicemail
 Vermont Mini-Lessons: Leaving A Voicemail Leaving a Voice Mail Message Learning Objective 1) When to leave a message 2) How to leave a message Materials: 1) Voice Mail Template blanks & samples 2) Phone
Vermont Mini-Lessons: Leaving A Voicemail Leaving a Voice Mail Message Learning Objective 1) When to leave a message 2) How to leave a message Materials: 1) Voice Mail Template blanks & samples 2) Phone
Guide to Health Insurance Part II: How to access your benefits and services.
 Guide to Health Insurance Part II: How to access your benefits and services. 1. I applied for health insurance, now what? Medi-Cal Applicants If you applied for Medi-Cal it will take up to 45 days to find
Guide to Health Insurance Part II: How to access your benefits and services. 1. I applied for health insurance, now what? Medi-Cal Applicants If you applied for Medi-Cal it will take up to 45 days to find
Grow healthy. Stay healthy. Grow healthy. Stay healthy. www.startsmartforyourbaby.com PREGNANCY JOURNEY BOOK DIARIO DEL EMBARAZO
 www.startsmartforyourbaby.com PREGNANCY JOURNEY BOOK 2012 Start Smart for Your Baby. All rights reserved. TM 2012 Start Smart for Your Baby. All rights reserved. TM DIARIO DEL EMBARAZO www.startsmartforyourbaby.com
www.startsmartforyourbaby.com PREGNANCY JOURNEY BOOK 2012 Start Smart for Your Baby. All rights reserved. TM 2012 Start Smart for Your Baby. All rights reserved. TM DIARIO DEL EMBARAZO www.startsmartforyourbaby.com
TEXAS STATE TEACHERS ASSOCIATION
 TEXAS STATE TEACHERS ASSOCIATION You have more to offer your child than you think. Thanks to your hard work and sacrifice, your child is enrolled in a Texas public school a learning environment that can
TEXAS STATE TEACHERS ASSOCIATION You have more to offer your child than you think. Thanks to your hard work and sacrifice, your child is enrolled in a Texas public school a learning environment that can
Northwestern University, Feinberg School of Medicine
 Improving Rates of Repeat Colorectal Cancer Screening Appendix Northwestern University, Feinberg School of Medicine Contents Patient Letter Included with Mailed FIT... 3 Automated Phone Call... 4 Automated
Improving Rates of Repeat Colorectal Cancer Screening Appendix Northwestern University, Feinberg School of Medicine Contents Patient Letter Included with Mailed FIT... 3 Automated Phone Call... 4 Automated
 LOS ANGELES UNIFIED SCHOOL DISTRICT STUDENT EMERGENCY INFORMATION FORM Parent Information: Please fill out completely and sign where indicated. In a major emergency, it is school district policy to retain
LOS ANGELES UNIFIED SCHOOL DISTRICT STUDENT EMERGENCY INFORMATION FORM Parent Information: Please fill out completely and sign where indicated. In a major emergency, it is school district policy to retain
OJO: Todos los formularios deberán llenarse en inglés. De lo contrario, no se le permitirá presentar sus documentos ante la Secretaría del Tribunal.
 OJO: Todos los formularios deberán llenarse en inglés. De lo contrario, no se le permitirá presentar sus documentos ante la Secretaría del Tribunal. For Clerk s Use Only (Para uso de la Secretaria solamente)
OJO: Todos los formularios deberán llenarse en inglés. De lo contrario, no se le permitirá presentar sus documentos ante la Secretaría del Tribunal. For Clerk s Use Only (Para uso de la Secretaria solamente)
SFGH FHC Healthy Children Vaccination Program Frequently Asked Questions
 SFGH FHC Healthy Children Vaccination Program Frequently Asked Questions The Family Health Center (FHC) Healthy Children Vaccination Program at SF General Hospital (SFGH) provides immunization services
SFGH FHC Healthy Children Vaccination Program Frequently Asked Questions The Family Health Center (FHC) Healthy Children Vaccination Program at SF General Hospital (SFGH) provides immunization services
Bienvenidos a Primer Grado Welcome to first grade
 Bienvenidos a Primer Grado Welcome to first grade Mrs. Pulido Mrs. Howard Mrs. Escamilla Maestras del programa doble sendero Dual Language Teachers En la mañana Morning Procedures El desayuno se sirve
Bienvenidos a Primer Grado Welcome to first grade Mrs. Pulido Mrs. Howard Mrs. Escamilla Maestras del programa doble sendero Dual Language Teachers En la mañana Morning Procedures El desayuno se sirve
Si tiene cualquier pregunta llame a su trabajadora de CCAP al número de teléfono indicado abajo. Boulder County Child Care Assistance Program
 Child Care Assistance Program Búsqueda de Trabajo Usted ha pedido cuidado para sus niños mientras busca trabajo a través del programa de CCAP. Este programa ofrece un total de 30 días mientras busca trabajo.
Child Care Assistance Program Búsqueda de Trabajo Usted ha pedido cuidado para sus niños mientras busca trabajo a través del programa de CCAP. Este programa ofrece un total de 30 días mientras busca trabajo.
SOLICITUD DE FAMILIA
 SOLICITUD DE FAMILIA DETALLES DE LA FAMILIA ABOUT YOUR FAMILY Apellidos (Padre) Father's family name(s) Nombres Christian names Apellidos (Madre) Mother's family name(s) Nombres Christian names Dirección
SOLICITUD DE FAMILIA DETALLES DE LA FAMILIA ABOUT YOUR FAMILY Apellidos (Padre) Father's family name(s) Nombres Christian names Apellidos (Madre) Mother's family name(s) Nombres Christian names Dirección
Welcome to lesson 2 of the The Spanish Cat Home learning Spanish course.
 Welcome to lesson 2 of the The Spanish Cat Home learning Spanish course. Bienvenidos a la lección dos. The first part of this lesson consists in this audio lesson, and then we have some grammar for you
Welcome to lesson 2 of the The Spanish Cat Home learning Spanish course. Bienvenidos a la lección dos. The first part of this lesson consists in this audio lesson, and then we have some grammar for you
I understand that I must request that this waiver be reconsidered annually, each school year. Parent/Guardian Signature: Date:
 Page 1 of 7 PARENTAL EXCEPTION WAIVER EDUCATION CODE 311(a): Children who know English (Exhibit 1) Name: School: Grade: Date of Birth: Language Designation: My child possesses good English language skills
Page 1 of 7 PARENTAL EXCEPTION WAIVER EDUCATION CODE 311(a): Children who know English (Exhibit 1) Name: School: Grade: Date of Birth: Language Designation: My child possesses good English language skills
GUIDE FOR PARENT TEACHER CONFERENCES
 GUIDE FOR PARENT TEACHER CONFERENCES A parent-teacher conference is a chance for you and your child s teacher to talk. You can talk about how your child is learning at home and at school. This list will
GUIDE FOR PARENT TEACHER CONFERENCES A parent-teacher conference is a chance for you and your child s teacher to talk. You can talk about how your child is learning at home and at school. This list will
HOMEWORK HELP PROGRAM STUDENT REQUIREMENTS STUDENT GUIDELINES
 HOMEWORK HELP PROGRAM This program is a cooperative learning experience shared between high school and elementary school students in the East Ramapo Central School District. It is designed to match Elementary
HOMEWORK HELP PROGRAM This program is a cooperative learning experience shared between high school and elementary school students in the East Ramapo Central School District. It is designed to match Elementary
University of Tennessee College of Medicine Chattanooga/Erlanger Health System 960 East Third Street Chattanooga, Tennessee 37403
 1 University of Tennessee College of Medicine Chattanooga/Erlanger Health System 960 East Third Street Chattanooga, Tennessee 37403 REMOVE THIS FIRST PAGE PRIOR TO GIVING CONSENT TO THE POTENTIAL SUBJECT.
1 University of Tennessee College of Medicine Chattanooga/Erlanger Health System 960 East Third Street Chattanooga, Tennessee 37403 REMOVE THIS FIRST PAGE PRIOR TO GIVING CONSENT TO THE POTENTIAL SUBJECT.
Creating your Single Sign-On Account for the PowerSchool Parent Portal
 Creating your Single Sign-On Account for the PowerSchool Parent Portal Welcome to the Parent Single Sign-On. What does that mean? Parent Single Sign-On offers a number of benefits, including access to
Creating your Single Sign-On Account for the PowerSchool Parent Portal Welcome to the Parent Single Sign-On. What does that mean? Parent Single Sign-On offers a number of benefits, including access to
Nombre de la persona completando esta forma
 mbre de Paciente mbre de la persona completando esta forma Fecha Relación del paciente / / Sexo Masculino Raza Numero de Seguro Social Fecha de Nacimiento Femenino / / / / POR FAVOR LISTE TODA LA GENTE
mbre de Paciente mbre de la persona completando esta forma Fecha Relación del paciente / / Sexo Masculino Raza Numero de Seguro Social Fecha de Nacimiento Femenino / / / / POR FAVOR LISTE TODA LA GENTE
HCHS/SOL Visit 2- Pregnancy Complications History
 Public reporting burden for this collection of information is estimated to average 06 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and
Public reporting burden for this collection of information is estimated to average 06 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and
For Parents and Caregivers
 Who Qualifies How to Enroll WHO QUALIFIES FOR WIC: HOW TO ENROLL IN WIC: You must Bring the infant or child to the WIC office to complete initial enrollment. If the infant or child can t be there because
Who Qualifies How to Enroll WHO QUALIFIES FOR WIC: HOW TO ENROLL IN WIC: You must Bring the infant or child to the WIC office to complete initial enrollment. If the infant or child can t be there because
An explanation by Sr. Jordan
 & An explanation by Sr. Jdan direct object pronouns We usually use Direct Object Pronouns to substitute f it them in a sentence when the it them follows the verb. Because of gender, him and her could also
& An explanation by Sr. Jdan direct object pronouns We usually use Direct Object Pronouns to substitute f it them in a sentence when the it them follows the verb. Because of gender, him and her could also
Screener for Peer Supporters
 Screener for Peer Supporters Primary Recruiter: Secondary Recruiter: Potential Peer Supporter Name: Phone #1: Home/Cell Phone #2: Home/Cell Address: City: Zip: Contact 1: Date: / / Contact 2: Date: / /
Screener for Peer Supporters Primary Recruiter: Secondary Recruiter: Potential Peer Supporter Name: Phone #1: Home/Cell Phone #2: Home/Cell Address: City: Zip: Contact 1: Date: / / Contact 2: Date: / /
Ausentismo (Truancy - Why it's important to go to school)
") Ausentismo (Truancy - Why it's important to go to school) By Jesus Villasenor-Ochoa Reproduced with permission of the University of MN 2003 BRYCS is a project of the United States Conference of Catholic
Ausentismo (Truancy - Why it's important to go to school) By Jesus Villasenor-Ochoa Reproduced with permission of the University of MN 2003 BRYCS is a project of the United States Conference of Catholic
Tres componentes importantes del programa Título I El propósito del Título I es de asegurar que todos los estudiantes tengan la oportunidad de
 Qué es Titulo I? El programa Título I para la Educación Primaria y Secundaria es el programa educacional más grande que recibe fondos federales El gobierno federal proporciona asistencia financiera a las
Qué es Titulo I? El programa Título I para la Educación Primaria y Secundaria es el programa educacional más grande que recibe fondos federales El gobierno federal proporciona asistencia financiera a las
Setting Up an Apple ID for your Student
 Setting Up an Apple ID for your Student You will receive an email from Apple with the subject heading of AppleID for Students Parent/Guardian Information Open the email. Look for two important items in
Setting Up an Apple ID for your Student You will receive an email from Apple with the subject heading of AppleID for Students Parent/Guardian Information Open the email. Look for two important items in
MajestaCare Healthy Baby Program
 MajestaCare Healthy Baby Program Helping you have a healthy baby Para que tenga un bebé saludable Your baby s provider After your baby becomes a member of MajestaCare health plan, you will get a letter
MajestaCare Healthy Baby Program Helping you have a healthy baby Para que tenga un bebé saludable Your baby s provider After your baby becomes a member of MajestaCare health plan, you will get a letter
LOS ANGELES UNIFIED SCHOOL DISTRICT OFFICE OF PERMITS AND STUDENT TRANSERS
 INTER-DISTRICT PERMIT APPEALS If your inter-district permit application has been denied cancelled, or revoked, you may appeal the decision if you believe that an exception to district policy is warranted
INTER-DISTRICT PERMIT APPEALS If your inter-district permit application has been denied cancelled, or revoked, you may appeal the decision if you believe that an exception to district policy is warranted
The Home Language Survey (HLS) and Identification of Students
 and Identification of Students") The Home Language Survey (HLS) and Identification of Students The Home Language Survey (HLS) is the document used to determine a student that speaks a language other than English. Identification of a language
The Home Language Survey (HLS) and Identification of Students The Home Language Survey (HLS) is the document used to determine a student that speaks a language other than English. Identification of a language
Escuela Alvarado. Paquete para Aplicación de AVID
 Escuela Alvarado Paquete para Aplicación de AVID Paquete incluye: Folleto de AVID Aplicación para el estudiante Información sobre la entrevista y carpeta Solicitud de calificaciones Información sobre ensayo
Escuela Alvarado Paquete para Aplicación de AVID Paquete incluye: Folleto de AVID Aplicación para el estudiante Información sobre la entrevista y carpeta Solicitud de calificaciones Información sobre ensayo
Student and Adult Release Forms
 Student and Adult Release Forms The following sample release forms are provided along with an explanation of the forms and your responsibility. For Tasks 3 and 4, your response will be based, in part,
Student and Adult Release Forms The following sample release forms are provided along with an explanation of the forms and your responsibility. For Tasks 3 and 4, your response will be based, in part,
Learning Masters. Early: Animal Bodies
 Learning Masters Early: Animal Bodies WhatILearned What important things did you learn in this theme? I learned that I learned that I learned that 22 Animal Bodies Learning Masters How I Learned Good readers
Learning Masters Early: Animal Bodies WhatILearned What important things did you learn in this theme? I learned that I learned that I learned that 22 Animal Bodies Learning Masters How I Learned Good readers
CUESTIONARIO DISEÑADO PARA EVALUAR EL PRODUCTO DESCUBRE LAS PALMAS DE GC! QUE SERÁ ADMINISTRADO A TRAVÉS DE LA WEB CREADA PARA EL PRODUCTO.
 ANEXO E. CUESTIONARIO DISEÑADO PARA EVALUAR EL PRODUCTO DESCUBRE LAS PALMAS DE GC! QUE SERÁ ADMINISTRADO A TRAVÉS DE LA WEB CREADA PARA EL PRODUCTO. CUESTIONARIO: El proyecto Descubre Las Palmas de GC!
ANEXO E. CUESTIONARIO DISEÑADO PARA EVALUAR EL PRODUCTO DESCUBRE LAS PALMAS DE GC! QUE SERÁ ADMINISTRADO A TRAVÉS DE LA WEB CREADA PARA EL PRODUCTO. CUESTIONARIO: El proyecto Descubre Las Palmas de GC!
RENT CONTROL BOARD OF THE TOWN OF WEST NEW YORK, N.J. 428-60 TH STREET WEST NEW YORK, N.J. 07093-2231 (201) 295-5290/91/92
 295-5290/91/92") FELIX E. ROQUE, MD MAYOR DEPT. OF PUBLIC AFFAIRS RENT CONTROL BOARD RENTAL AGREEMENT APPLICATION NAME OF ADDRESS OF LANDLORD: PROPERTY ADDRESS: APARTMENT #: 3 COPIES (1) Original rental agreement signed
FELIX E. ROQUE, MD MAYOR DEPT. OF PUBLIC AFFAIRS RENT CONTROL BOARD RENTAL AGREEMENT APPLICATION NAME OF ADDRESS OF LANDLORD: PROPERTY ADDRESS: APARTMENT #: 3 COPIES (1) Original rental agreement signed
I am the parent or legal guardian of.
 EXHIBIT Descriptive Code: IFCB-R/E (2) FIELD TRIPS AND EXCURSIONS Date: March 9, 2006 Clarke County School District Student Travel Authorization and Teacher ation Form To SCHOOL: I am the parent or legal
EXHIBIT Descriptive Code: IFCB-R/E (2) FIELD TRIPS AND EXCURSIONS Date: March 9, 2006 Clarke County School District Student Travel Authorization and Teacher ation Form To SCHOOL: I am the parent or legal
Financial Affidavit for Child Support, DC 6:5(2) Declaración Jurada de Finanzas para Manutención de Menores, DC 6:5(2).
 Declaración Jurada de Finanzas para Manutención de Menores, DC 6:5(2).") IN THE DISTRICT CURT F CUNTY, NEBRASKA (county where Complaint filed) EN LA CRTE DE DISTRIT DEL CNDAD DE, NEBRASKA (condado donde se entabló la Demanda), ) (your full name) (su nombre completo) ) Plaintiff,/
IN THE DISTRICT CURT F CUNTY, NEBRASKA (county where Complaint filed) EN LA CRTE DE DISTRIT DEL CNDAD DE, NEBRASKA (condado donde se entabló la Demanda), ) (your full name) (su nombre completo) ) Plaintiff,/
Adult Application 18 and over ONLY ******************************** Aplicación de Adultos Solo para mayores de 18 años
 Adult Application 18 and over ONLY ******************************** Aplicación de Adultos Solo para mayores de 18 años FREE GRATIS Beacon Programs Adult Enrollment Form Beacon PROGRAMS Participant Information
Adult Application 18 and over ONLY ******************************** Aplicación de Adultos Solo para mayores de 18 años FREE GRATIS Beacon Programs Adult Enrollment Form Beacon PROGRAMS Participant Information
Spanish Version provided Below
 Spanish Version provided Below Greater Waltown United Holy Church s Summer Reading and Math Program 706 Belvin Avenue Durham, N. C. 27712 (919) 220-7087 May 3, 2015 Dear Parent/Guardian: Summer can be
Spanish Version provided Below Greater Waltown United Holy Church s Summer Reading and Math Program 706 Belvin Avenue Durham, N. C. 27712 (919) 220-7087 May 3, 2015 Dear Parent/Guardian: Summer can be
Welcome to the CU at School Savings Program!
 Welcome to the CU at School Savings Program! Thank you for your interest in Yolo Federal Credit Union s CU at School savings program. This packet of information has everything you need to sign your child
Welcome to the CU at School Savings Program! Thank you for your interest in Yolo Federal Credit Union s CU at School savings program. This packet of information has everything you need to sign your child
Voter Information Guide and Sample Ballot
 Voter Information Guide and Sample Ballot Special Election San Bernardino Mountains Community Hospital District Tuesday, June 4, 2013 Elections Office of the Registrar of Voters 777 East Rialto Ave. San
Voter Information Guide and Sample Ballot Special Election San Bernardino Mountains Community Hospital District Tuesday, June 4, 2013 Elections Office of the Registrar of Voters 777 East Rialto Ave. San
Improving Rates of Colorectal Cancer Screening Among Never Screened Individuals
 Improving Rates of Colorectal Cancer Screening Among Never Screened Individuals Northwestern University, Feinberg School of Medicine Contents Patient Letter Included with Mailed FIT... 3 Automated Phone
Improving Rates of Colorectal Cancer Screening Among Never Screened Individuals Northwestern University, Feinberg School of Medicine Contents Patient Letter Included with Mailed FIT... 3 Automated Phone
EL ESTILO INDIRECTO (REPORTED SPEECH)
") EL ESTILO INDIRECTO () **El estilo indirecto es la forma de reproducir en tercera persona lo que alguien ha dicho textualmente. I m tired she said. She said that she was tired. Como se observa en el ejemplo
EL ESTILO INDIRECTO () **El estilo indirecto es la forma de reproducir en tercera persona lo que alguien ha dicho textualmente. I m tired she said. She said that she was tired. Como se observa en el ejemplo
 Aula Inglés SOLICITUD FAMILIA para AU PAIRS - FAMILY APPLICATION for AU PAIRS DETALLES DE CONTACTO -CONTACT DETAILS Nombre /Full Name Dirección/Address FOTO/PHOTO Provincia / Region Ciudad - City: País/Country
Aula Inglés SOLICITUD FAMILIA para AU PAIRS - FAMILY APPLICATION for AU PAIRS DETALLES DE CONTACTO -CONTACT DETAILS Nombre /Full Name Dirección/Address FOTO/PHOTO Provincia / Region Ciudad - City: País/Country
Affordable Care Act Informative Sessions and Open Enrollment Event
 2600 Cedar Ave., P.O. Box 2337, Laredo, TX 78044 Hector F. Gonzalez, M.D., M.P.H Tel. (956) 795-4901 Fax. (956) 726-2632 Director of Health News Release. Date: February 9, 2015 FOR IMMEDIATE RELEASE To:
2600 Cedar Ave., P.O. Box 2337, Laredo, TX 78044 Hector F. Gonzalez, M.D., M.P.H Tel. (956) 795-4901 Fax. (956) 726-2632 Director of Health News Release. Date: February 9, 2015 FOR IMMEDIATE RELEASE To:
DEPARTAMENTO ESTATAL DE SERVICIOS DE SALUD DE TEXAS
 DEPARTAMENTO ESTATAL DE SERVICIOS DE SALUD DE TEXAS DAVID L. LAKEY, M.D. DIRECTOR P.O. Box 149347 Austin, Texas 78714-9347 1-888-963-7111 TTY (teletipo): 1-800-735-2989 www.dshs.state.tx.us 1 de marzo,
DEPARTAMENTO ESTATAL DE SERVICIOS DE SALUD DE TEXAS DAVID L. LAKEY, M.D. DIRECTOR P.O. Box 149347 Austin, Texas 78714-9347 1-888-963-7111 TTY (teletipo): 1-800-735-2989 www.dshs.state.tx.us 1 de marzo,
PODER NOTARIAL DE UN MENOR DE EDAD
 POWER OF ATTORNEY OVER A MINOR PODER NOTARIAL DE UN MENOR DE EDAD PUEDE USAR ESTE PAQUETE SÓLO SI SE CUMPLEN TODAS LAS SIGUIENTES CONDICIONES:! Usted desea dar autoridad temporal sobre su hijo a otra persona.!
POWER OF ATTORNEY OVER A MINOR PODER NOTARIAL DE UN MENOR DE EDAD PUEDE USAR ESTE PAQUETE SÓLO SI SE CUMPLEN TODAS LAS SIGUIENTES CONDICIONES:! Usted desea dar autoridad temporal sobre su hijo a otra persona.!
ESL Parent Meeting. Itasca School District 10 Benson Primary School Franzen Intermediate School Peacock Middle School
 ESL Parent Meeting Itasca School District 10 Benson Primary School Franzen Intermediate School Peacock Middle School The Program Two ESL Teachers Pull out method (Grades K-8) 30 minutes per day 5 days
ESL Parent Meeting Itasca School District 10 Benson Primary School Franzen Intermediate School Peacock Middle School The Program Two ESL Teachers Pull out method (Grades K-8) 30 minutes per day 5 days
MANUAL EASYCHAIR. A) Ingresar su nombre de usuario y password, si ya tiene una cuenta registrada Ó
 Ingresar su nombre de usuario y password, si ya tiene una cuenta registrada Ó") MANUAL EASYCHAIR La URL para enviar su propuesta a la convocatoria es: https://easychair.org/conferences/?conf=genconciencia2015 Donde aparece la siguiente pantalla: Se encuentran dos opciones: A) Ingresar
MANUAL EASYCHAIR La URL para enviar su propuesta a la convocatoria es: https://easychair.org/conferences/?conf=genconciencia2015 Donde aparece la siguiente pantalla: Se encuentran dos opciones: A) Ingresar
Learning Masters. Early: Food From Plants
 Learning Masters Early: Food From Plants WhatILearned What important things did you learn in this theme? I learned that I learned that I learned that 22 Food From Plants Learning Masters How I Learned
Learning Masters Early: Food From Plants WhatILearned What important things did you learn in this theme? I learned that I learned that I learned that 22 Food From Plants Learning Masters How I Learned
Connection from School to Home Science Grade 5 Unit 1 Living Systems
 Connection from School to Home Science Grade 5 Unit 1 Living Systems Here is an activity to help your child understand human body systems. Here is what you do: 1. Look at the pictures of the systems that
Connection from School to Home Science Grade 5 Unit 1 Living Systems Here is an activity to help your child understand human body systems. Here is what you do: 1. Look at the pictures of the systems that
ANNUAL REPORT OF GUARDIAN ON CONDITION OF WARD/INCAPACITATED PERSON INFORME ANUAL DEL TUTOR SOBRE LA CONDICIÓN DEL PUPILO/PERSONA INCAPACITADA/INHÁBIL
 Nebraska State Court Form REQUIRED Formulario del Tribunal del Estado de Nebraska REQUERIDO ANNUAL REPORT OF GUARDIAN ON CONDITION OF WARD/INCAPACITATED PERSON INFORME ANUAL DEL TUTOR SOBRE LA CONDICIÓN
Nebraska State Court Form REQUIRED Formulario del Tribunal del Estado de Nebraska REQUERIDO ANNUAL REPORT OF GUARDIAN ON CONDITION OF WARD/INCAPACITATED PERSON INFORME ANUAL DEL TUTOR SOBRE LA CONDICIÓN
\RESOURCE\ELECTION.S\PROXY.CSP
 The following is an explanation of the procedures for calling a special meeting of the shareholders. Enclosed are copies of documents, which you can use for your meeting. If you have any questions about
The following is an explanation of the procedures for calling a special meeting of the shareholders. Enclosed are copies of documents, which you can use for your meeting. If you have any questions about
Golden Valley High School English Language Advisory Council (ELAC) Meeting Agenda Tuesday, September 1, 2015
 Meeting Agenda Tuesday, September 1, 2015") English Language Advisory Council (ELAC) Meeting Agenda Tuesday, September 1, 2015 1. Welcome and Introductions a. Mrs. Jennifer Ambrose: Administrator b. Mrs. Arian Wilson: ELD Coordinator, ELL & Study
English Language Advisory Council (ELAC) Meeting Agenda Tuesday, September 1, 2015 1. Welcome and Introductions a. Mrs. Jennifer Ambrose: Administrator b. Mrs. Arian Wilson: ELD Coordinator, ELL & Study
Student Violence, Bullying, Intimidation, Harassment
 Case 4:74-cv-00090-DCB Document 1690-6 Filed 10/01/14 Page 159 of 229 Student Violence, Bullying, Intimidation, Harassment COMPLAINT FORM (To be filed with any School District employee who will forward
Case 4:74-cv-00090-DCB Document 1690-6 Filed 10/01/14 Page 159 of 229 Student Violence, Bullying, Intimidation, Harassment COMPLAINT FORM (To be filed with any School District employee who will forward
Registro de Semilla y Material de Plantación
 Registro de Semilla y Material de Plantación Este registro es para documentar la semilla y material de plantación que usa, y su estatus. Mantenga las facturas y otra documentación pertinente con sus registros.
Registro de Semilla y Material de Plantación Este registro es para documentar la semilla y material de plantación que usa, y su estatus. Mantenga las facturas y otra documentación pertinente con sus registros.
Going Home. Medicines. Pain. Diet
 Going Home After an illness or injury, some things may change in your life. Make sure you and your family know the answers to these questions before you go home from the hospital. Medicines Am I taking
Going Home After an illness or injury, some things may change in your life. Make sure you and your family know the answers to these questions before you go home from the hospital. Medicines Am I taking
The ADE Direct Certification User Guide is a tool for authorized ADE and school district personnel to use in conjunction with the ADE Direct
 The ADE Direct Certification User Guide is a tool for authorized ADE and school district personnel to use in conjunction with the ADE Direct Certification website. 1 This User Guide is a reference guide
The ADE Direct Certification User Guide is a tool for authorized ADE and school district personnel to use in conjunction with the ADE Direct Certification website. 1 This User Guide is a reference guide
Lista 1. Nombre. Lista 5. Lista 4 Lista 3 Lista 2. Lista 1. Lista 10. Lista 9. Lista 8. Lista 7. Lista 6
 Nombre Lista 1 Lista 10 Lista 9 Lista 8 Lista 7 Lista 6 Lista 5 Lista 4 Lista 3 Lista 2 Lista 1 Yo (I) Y (and) Un (a, an) Una (a-for female) Veo (I see) Mi (my) Tu (you) A (to) Al (to) Así (like this)
Nombre Lista 1 Lista 10 Lista 9 Lista 8 Lista 7 Lista 6 Lista 5 Lista 4 Lista 3 Lista 2 Lista 1 Yo (I) Y (and) Un (a, an) Una (a-for female) Veo (I see) Mi (my) Tu (you) A (to) Al (to) Así (like this)
Family Criteria Questionnaire
 Office Use Only: Program Code: HS STPK ECBG ECSE FL KS Entry Date: US Entry Date: B/C (I 94) on file? Y/N State/Country Family Criteria Questionnaire Child must be 3 or 4 years of age by August 31, 2014
Office Use Only: Program Code: HS STPK ECBG ECSE FL KS Entry Date: US Entry Date: B/C (I 94) on file? Y/N State/Country Family Criteria Questionnaire Child must be 3 or 4 years of age by August 31, 2014
ACCESS for ELLs, a Test of English Proficiency. El ACCESS de los estudiantes ELL, una prueba de conocimientos de inglés
 ACCESS for ELLs, a Test of English Proficiency El ACCESS de los estudiantes ELL, una prueba de conocimientos de inglés The ACCESS for ELLs Test This test: ê shows how well your child is learning English;
ACCESS for ELLs, a Test of English Proficiency El ACCESS de los estudiantes ELL, una prueba de conocimientos de inglés The ACCESS for ELLs Test This test: ê shows how well your child is learning English;
MY Escuelas Saludables Forma de Autorización de Padres
 MY Escuelas Saludables Forma de Autorización de Padres Firmando esta forma, Yo doy consentimiento para que mi hijo tenga acceso a algún o todos los servicios disponibles de MY Escuelas Saludables, siempre
MY Escuelas Saludables Forma de Autorización de Padres Firmando esta forma, Yo doy consentimiento para que mi hijo tenga acceso a algún o todos los servicios disponibles de MY Escuelas Saludables, siempre
Reglamento 723-4 ESTUDIANTES 13 de junio de 2007 ESTUDIANTES. Requisitos para el examen de tuberculosis
 13 de junio de 2007 Requisitos para el examen de tuberculosis Todos aquellos estudiantes de edad preescolar, escolar, o adultos, que estén intentando ingresar a las Escuelas Públicas del Condado de Prince
13 de junio de 2007 Requisitos para el examen de tuberculosis Todos aquellos estudiantes de edad preescolar, escolar, o adultos, que estén intentando ingresar a las Escuelas Públicas del Condado de Prince
PRUEBA DE INGLÉS SECUNDARIA
 Dirección General de Ordenación Académica e Innovación Educativa PRUEBA DE INGLÉS SECUNDARIA EXPRESIÓN ORAL AUTOAPLICACIÓN EVALUACIÓN DIAGNÓSTICA SECUNDARIA 2007 Servicio de Evaluación y Calidad Educativa
Dirección General de Ordenación Académica e Innovación Educativa PRUEBA DE INGLÉS SECUNDARIA EXPRESIÓN ORAL AUTOAPLICACIÓN EVALUACIÓN DIAGNÓSTICA SECUNDARIA 2007 Servicio de Evaluación y Calidad Educativa
PB #11-111-OPE. Attachment: Please use Print on M-687r Referral to Treatment Program (Rev. 11/30/11) (Rev. 11/30/11)
 (Rev. 11/30/11)") FAMILY INDEPENDENCE ADMINISTRATION Matthew Brune, Executive Deputy Commissioner James K. Whelan, Deputy Commissioner Policy, Procedures, and Training Stephen Fisher, Assistant Deputy Commissioner Office
FAMILY INDEPENDENCE ADMINISTRATION Matthew Brune, Executive Deputy Commissioner James K. Whelan, Deputy Commissioner Policy, Procedures, and Training Stephen Fisher, Assistant Deputy Commissioner Office
Instructor: Do you remember how to say the verb "to speak"? Instructor: How do you ask a friend Do you speak Spanish?
 Learning Spanish Like Crazy Spoken Spanish Lección Dos. Listen to the following conversation: Male: Hablas inglés? Female: Sí, hablo inglés porque practico todos los días. Male: Dónde? Female: Practico
Learning Spanish Like Crazy Spoken Spanish Lección Dos. Listen to the following conversation: Male: Hablas inglés? Female: Sí, hablo inglés porque practico todos los días. Male: Dónde? Female: Practico
Portal para Padres CPS - Parent Portal. Walter L. Newberry Math & Science Academy Linda Foley-Acevedo, Principal Ed Collins, Asst.
 Portal para Padres CPS - Parent Portal Walter L. Newberry Math & Science Academy Linda Foley-Acevedo, Principal Ed Collins, Asst. Principal (773) 534-8000 Formando su cuenta - Setting up your account Oprima
Portal para Padres CPS - Parent Portal Walter L. Newberry Math & Science Academy Linda Foley-Acevedo, Principal Ed Collins, Asst. Principal (773) 534-8000 Formando su cuenta - Setting up your account Oprima
Some examples. I wash my clothes, I wash the dishes, I wash the car, I wash the windows. I wash my hands, I wash my hair, I wash my face.
 Reflexive verbs In this presentation, we are going to look at a special group of verbs called reflexives. Let s start out by thinking of the English verb wash. List several things that you can wash. Some
Reflexive verbs In this presentation, we are going to look at a special group of verbs called reflexives. Let s start out by thinking of the English verb wash. List several things that you can wash. Some
Disfruten su verano! Hola estudiantes,
 Hola estudiantes, We hope that your experience during Spanish 1 was enjoyable and that you are looking forward to improving your ability to communicate in Spanish. As we all know, it is very difficult
Hola estudiantes, We hope that your experience during Spanish 1 was enjoyable and that you are looking forward to improving your ability to communicate in Spanish. As we all know, it is very difficult
English Literacy Success Team, e3 Civic High October 30, 2014
 English Literacy Success Team, e3 Civic High October 30, 2014 What is the English Language Success Team? The purpose of our committee is to provide an open conversation between parents, students, and teachers
English Literacy Success Team, e3 Civic High October 30, 2014 What is the English Language Success Team? The purpose of our committee is to provide an open conversation between parents, students, and teachers
Learning Masters. Fluent: Wind, Water, and Sunlight
 Learning Masters Fluent: Wind, Water, and Sunlight What I Learned List the three most important things you learned in this theme. Tell why you listed each one. 1. 2. 3. 22 Wind, Water, and Sunlight Learning
Learning Masters Fluent: Wind, Water, and Sunlight What I Learned List the three most important things you learned in this theme. Tell why you listed each one. 1. 2. 3. 22 Wind, Water, and Sunlight Learning
FORMAT B2 SPEAKING EXAM
 FORMAT B2 SPEAKING EXAM PRODUCCIÓN ORAL 25% 1 2 3 El examinador, de manera alternativa, hará preguntas a los dos alumnos. (4-5 min en total) Cada candidato tiene 15 segundos para preparar un tema determinado
FORMAT B2 SPEAKING EXAM PRODUCCIÓN ORAL 25% 1 2 3 El examinador, de manera alternativa, hará preguntas a los dos alumnos. (4-5 min en total) Cada candidato tiene 15 segundos para preparar un tema determinado
Steps to Understand Your Child s Behavior. Customizing the Flyer
 Steps to Understand Your Child s Behavior Customizing the Flyer Hello! Here is the PDF Form Template for use in advertising Steps to Understanding Your Child s Behavior (HDS Behavior Level 1B). Because
Steps to Understand Your Child s Behavior Customizing the Flyer Hello! Here is the PDF Form Template for use in advertising Steps to Understanding Your Child s Behavior (HDS Behavior Level 1B). Because
TEESP: Technology Enhanced Elementary Spanish Program Lesson Planner. Title: Qué pasa con su corazón?
 : Technology Enhanced Elementary Spanish Program Lesson Plan #: 60 Story #: 2 Level 6 Resources used: Title: Qué pasa con su corazón? Pages/URL/etc.: Cuéntame! Pages 167-174 Objective(s) & Progress Indicator(s):
: Technology Enhanced Elementary Spanish Program Lesson Plan #: 60 Story #: 2 Level 6 Resources used: Title: Qué pasa con su corazón? Pages/URL/etc.: Cuéntame! Pages 167-174 Objective(s) & Progress Indicator(s):
Migrant. Learners Today LEADERS Tomorrow!
 Migrant Learners Today LEADERS Tomorrow! 2014 Migrant Summer Program Language Enrichment for English Language Learners Through Science Themes Students will enhance English language acquisition through
Migrant Learners Today LEADERS Tomorrow! 2014 Migrant Summer Program Language Enrichment for English Language Learners Through Science Themes Students will enhance English language acquisition through
Solicitud para el Programa de Child Care Subsidies and Referrals (CCSR)
") GAP CLIFF FRSFF SN Application for Child Care Subsidy and Referrals (CCSR) Program Parent/guardian info: Last Name: First Name: Middle Initial: Sex: Birth date: E-mail Address: Residence Address: City:
GAP CLIFF FRSFF SN Application for Child Care Subsidy and Referrals (CCSR) Program Parent/guardian info: Last Name: First Name: Middle Initial: Sex: Birth date: E-mail Address: Residence Address: City:
Learning Compact. Schools would agree to provide children every opportunity to learn in a supportive, drug- and violence-free environment.
 Learning Compact What is a learning compact? A learning compact is a voluntary agreement between the home and school. The agreement would define goals, expectations and shared responsibilities of schools
Learning Compact What is a learning compact? A learning compact is a voluntary agreement between the home and school. The agreement would define goals, expectations and shared responsibilities of schools
Formulario de Postulación Estudiante de Intercambio Application Form / Exchange Student
 Formulario de Postulación Estudiante de Intercambio Application Form / Exchange Student Información Personal Personal Information Nombres First Name Apellidos Last Name Dirección permanente Permanent Address
Formulario de Postulación Estudiante de Intercambio Application Form / Exchange Student Información Personal Personal Information Nombres First Name Apellidos Last Name Dirección permanente Permanent Address
Citizenship. Citizenship means obeying the rules and working to make your community a better place.
 Citizenship Citizenship means obeying the rules and working to make your community a better place. I show good citizenship when I help keep my school and community clean. I am a good citizen when I follow
Citizenship Citizenship means obeying the rules and working to make your community a better place. I show good citizenship when I help keep my school and community clean. I am a good citizen when I follow
Ethnography of a Classroom Sample Questions (May need to be adjusted for lower grades)
") Claremont Graduate University, Teacher Education Program Ethnography of a Classroom Sample Questions Parent/Family Interview Be sure to schedule enough time for interview minimum 30 minutes. If possible,
Claremont Graduate University, Teacher Education Program Ethnography of a Classroom Sample Questions Parent/Family Interview Be sure to schedule enough time for interview minimum 30 minutes. If possible,
Please read the questions below. If the answer to ANY of the questions is YES, please check this box
 TUBERCULOSIS QUESTIONNAIRE Student Name Date of Birth School Please read the following information and answer the questions below. This information will help determine if your child needs a TB skin test.
TUBERCULOSIS QUESTIONNAIRE Student Name Date of Birth School Please read the following information and answer the questions below. This information will help determine if your child needs a TB skin test.
Información del participante
 Formulario de Registracion Información del participante 1. 2. Primer nombre 3. Inicial del Segundo nombre 4. Numero de seguro social 5. Sexo 6. Fecha de nacimiento Masc. Fem. Mes Dia Año 7. Domicilio (numero
Formulario de Registracion Información del participante 1. 2. Primer nombre 3. Inicial del Segundo nombre 4. Numero de seguro social 5. Sexo 6. Fecha de nacimiento Masc. Fem. Mes Dia Año 7. Domicilio (numero