TRASPLANTE DE HIGADO Y VIH
|
|
|
- Julián Botella Martin
- hace 6 años
- Vistas:
Transcripción
1 IX CONGRESO DE LA ASOCIACION COLOMBIANA DE HEPATOLOGIA MEDELLIN - MARZO 9-11 DE 2017 TRASPLANTE DE HIGADO Y VIH JHON EDISON PRIETO ORTIZ HEPATOLOGO-GASTROENTEROLOGO-INTERNISTA ORGANIZACION SANITAS CLINICA COLOMBIA CENTRO DE ENFERMEDADES HEPATICAS Y DIGESTIVAS (CEHYD) BOGOTA. COLOMBIA
2 TEMAS A TRATAR Epidemiologia Como se comporta la enfermedad hepatica en el paciente con VIH Indicacion de trasplante en VIH cuando? Resultados Futuro con los nuevos antivirales Conclusiones
3 EPIDEMIOLOGIA
4 EPIDEMIOLOGIA DEL VIH/SIDA EN EL MUNDO ,7 millones de adultos y niños con el VIH / SIDA 17,4 millones de mujeres. 3,3 millones de niños con el VIH / SIDA en todo el mundo 2,1 millones de personas infectadas con el VIH en ese año 1.1 millones de personas murieron de SIDA en ese año Prevalencia general del VIH estable o aumentado en algunos países (> supervivencia- tratamiento antirretroviral). Incidencia de nuevas infecciones disminuyó 38 % desde En 2013 en todo el mundo, el VIH / SIDA una de las diez principales causas de muerte (mortalidad asociada con el VIH en el África subsahariana, donde fue la principal causa). UNAIDS. Global AIDS update, Joint United Nations Programme on VIH/AIDS. The Gap Report. September GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, : a systematic analysis for the Global Burden of Disease Study Lancet 2015; 385:117.
5 EPIDEMIOLOGIA DEL VIH/SIDA EN COLOMBIA personas aprox. viven con el VIH adultos(> 15 años). Prevalencia en adultos entre 15 y 49 años 0.5% Mujeres de al menos 15 años Niños de 0 a 14 años, viven con el VIH Fallecimientos por sida Huérfanos por el sida de 0 a 17 años UNAIDS. Global AIDS update, Joint United Nations Programme on VIH/AIDS. The Gap Report. September GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, : a systematic analysis for the Global Burden of Disease Study Lancet 2015; 385:117.
6 COMO SE COMPORTA LA ENFERMEDAD HEPATICA EN EL PACIENTE CON VIH
7 TERAPIA ANTIRETROVIRAL Año 1996, tratamiento antiretroviral de gran actividad (TARGA): disminuye morbilidad por procesos oportunistas y la mortalidad global de los pacientes con sida. Mocroft A, Brettle R, Kirk O, Blaxhult A, Parkin JM, Antunes F, Francioli P, D Arminio Monforte A, Fox Z, Lundgren JD. Changes in the cause of death among HIV positive subjects across Europe: results from the EuroSIDA study. AIDS 2002; 16: Weber R, Sabin CA, Friis-Møller N, Reiss P, El-Sadr WM, Kirk O, Dabis F, Law MG, Pradier C, De Wit S, Akerlund B, Calvo G, Monforte Ad, Rickenbach M, Ledergerber B, Phillips AN, Lundgren JD. Liverrelated deaths in persons infected with the human immunodeficiency virus: the D: A: D study. Arch Intern Med 2006; 166:
8 EFECTOS ADVERSO DE TARGA A LARGO PLAZO Toxicidad mitocondrial Diabetes M Enf cardiovascular Hepatotoxicidad Weber R, Sabin CA, Friis-Moller N, Reis P, El-Sadr WM, Kirk O, et al. Liver-related deaths in persons infected with the human immunodeficiency virus: the D:A:D study. Arch Int Med 2006;166:

9 ENFERMEDAD HEPATICA Y VIH Riesgo de muerte después del primer episodio de descompensación es más alto en los coinfectados VIH / VHC que en monoinfectados VHC. Medianas de supervivencia de 16 y 48 meses, respectivamente. Predictores de mortalidad : la edad, severidad de le enfermedad (MELD, CPT) y la naturaleza del evento de descompensación Estos pacientes deben referirse tempranamente para TX hepatico después del primer episodio de descompensación. Pineda JA, Romero-Gomez M, Diaz-Garcia F, Giron-Gonzalez JA, Montero JL, Torre-Cisneros J, et al. VIH coinfection shortens the survival of patients with hepatitis C virus-related decompensated cirrhosis. Hepatology 2005;41:
10 ENFERMEDAD HEPATICA Y VIH Pineda JA, Romero-Gomez M, Diaz-Garcia F, Giron-Gonzalez JA, Montero JL, Torre-Cisneros J, et al. VIH coinfection shortens the survival of patients with hepatitis C virus-related decompensated cirrhosis. Hepatology 2005;41:
11 ENFERMEDAD HEPATICA Y VIH Paciente VIH con ESLD en lista de espera tiene una mortalidad entre 36 y 60 %. Sobrevida del paciente VIH con ESLD es menor que controles no VIH MELD score factor independente de mortalidad. Los pacientes deben ser valorados precozmente para TOH. Miro JM, Murillas J, Laguno M et al. Natural history and prognosis of end stage liver disease (ESLD) in Spanish VIH-1 infected patients: a prospective cohort study of 104 patients ( ). 10th European AIDS Conference. Dublin, Ireland, November Abstr. PS7/1. Pineda JA, Romero-Gomez M, Diaz-Garcia F et al. VIH co-infection shortens the survival of patients with hepatitis C virusrelated decompensated cirrhosis. Hepatology, 2005, 41, Merchante N, Giron-Gonzalez JA, Gonzalez-Serrano M, et al. Survival and prognostic factors of VIH-infected patients with VHC-related end-stage liver disease. AIDS, 2006, 20, Maida I, Nunez M, Gonzalez-Lahoz J, Soriano V. Liver transplantation in VIH-VHC coinfected candidates: what is the most appropriate time for evaluation? AIDS Res Hum Retroviruses, 2005, 21, Ragni MV, Eghtesad B, Schlesinger KW et al. Pretransplant survival is shorter in VIH-positive than VIH-negative subjects with end-stage liver disease. Liver Transpl, 2005, 11,
 in Spanish VIH-1 infected patients: a prospective cohort study of 104 patients (1999 2004). 10th European AIDS Conference.")
12 SOBREVIDAS MENORES EN PACIENTES VIH CON ENFERMEDAD HEPATICA TERMINAL (ESLD) 39. Miro JM, Murillas J, Laguno M et al. Natural history and prognosis of end stage liver disease (ESLD) in Spanish VIH-1 infected patients: a prospective cohort study of 104 patients ( ). 10th European AIDS Conference. Dublin, Ireland, November Abstr. PS7/1. 40.Pineda JA, Romero-Gomez M, Diaz-Garcia F et al. VIH co-infection shortens the survival of patients with hepatitis C virus-related decompensated cirrhosis. Hepatology, 2005, 41,
. Murillas J, Rimola A, Laguno M, de Lazzari E, Rascón J, Aguëro F, Blanco JL, Moitinho E, Moreno A, Miró JM.")
13 104 pacientes, 2 centros Seguimiento promedio 10 meses Mortalidad a los 1, 2 y 3 años fue del 43%, 59% y 70% En análisis multivariado, el MELD y la incapacidad de alcanzar una carga viral indetectable del ARN del VIH-1 únicas variables asociadas con el riesgo de muerte (P 0,001). Murillas J, Rimola A, Laguno M, de Lazzari E, Rascón J, Aguëro F, Blanco JL, Moitinho E, Moreno A, Miró JM. The model for end-stage liver disease score is the best prognostic factor in human immunodeficiency virus 1-infected patients with end-stage liver disease: a prospective cohort study. Liver Transpl 2009; 15:

14 Subramanian A, Sulkowski M, Barin B, Stablein D, Curry M, Nissen N, et al. MELD score is an important predictor of pretransplantation mortality in HIV-infected liver transplant candidates. Gastroenterology 2010;138:
15 VIH -VHC COINFECCION Se afectan adversamente cada uno VIH : Acelera la progresion de la enfermedad VHC por Incremento de la viremia y hepatitis Inmunodeficiencia celular Incrementa riesgo de fibrosis y cirrosis Puede llevar a hepatitis colestática fibrosante VHC : Opuesto debatido Aumenta toxicidad antiretroviral y disminuye su efectividad Vallet-Pichard A, Pol S. Natural history and predictors of severity of chronic hepatitis C virus (VHC) and human immunodeficiency virus (VIH) coinfection. J Hepatol 2006;44:S28 S34. Alberti A, Clumeck N, Collins S, Gerlich W, Lundgren J, Palu` G, et al. Short statement of the first European consensus conference on the treatment of chronic hepatitis B and C in VIH co-infected patients. J Hepatol 2005;42: Rockstroh JK, Mocroft A, Soriano V, Tural C, Losso MH, Horban A, et al. Influence of hepatitis C virus infection on VIH-1 disease progression and response to highly active antiretroviral therapy. J Infect Dis 2005;192: Greub G, Ledergerber B, Battegay M, Grob P, Perrin L, Furrer H, et al. Clinical progression, survival, and immune recovery during antiretroviral therapy in patients with VIH-1 and hepatitis C virus coinfection: the Swiss VIH cohort study. Lancet 2000;356:
16 COINFECCION VIH -HBV VHB : No induce progresión del VIH o afecta su tratamiento, pero : Incrementa la mortalidad relacionada con hepatopatias en los coinfectados VIH : Morbilidad menor porque los nucleosidos y nucleotidos inhibidores de la transcriptasa inversa del VIH tambien suprimen el HBV Alberti A, Clumeck N, Collins S, Gerlich W, Lundgren J, Palu` G, et al. Short statement of the first European consensus conference on the treatment of chronic hepatitis B and C in VIH co-infected patients. J Hepatol 2005;42: Levy V, Grant RM. Antiretroviral therapy for hepatitis B virus- VIH-coinfected patients: promises and pitfalls. Clin Infect Dis 2006;43:
17 ENFERMEDAD HEPATICA TERMINAL EN PACIENTES VIH La enfermedad hepática terminal se ha convertido en una de las primeras causas de ingreso hospitalario y de muerte Staples CT, Rimland D, Dudas D. Hepatitis C in the VIH (human immunodeficiency virus) Atlanta V.A. (Veterans Affairs Medical Center) Cohort Study (HAVACS): the effect of coinfection on survival. Clin Infect Dis 1999;29: Soriano V, Sulkowski M, Bergin C, Hatzakis A, Cacoub P, Katlama C, et al.care of patients with chronic hepatitis C and VIH co-infection: recommendations from the VIH-VHC International Panel. AIDS 2002;16: Bica I, McGovern B, Dhar R, Stone D, McGowan K, Scheib R, et al. Increasing mortality due to end-stage liver disease in patients with human immunodeficiency virus infection. Clin Infect Dis 2001;32: Camino X, Iribarren JA, Arrizabalaga J, Rodríguez F, Von Wichmann AM. Causes of mortality among patients infected with the human immunodeficiency virus in the era of high active antiretroviral therapy. Enferm Infecc Microbiol Clin 2001;19:85-6.
18 CAUSAS DE MUERTE EN VIH Paises pobres % por infecciones oportunistas y malignidades Paises ricos D.A.D Cohorte, n= 1246 SIDA 31.1 % 14.5 % enfermedades hepáticas 11% enf cardiovasculares 9.4 % Malignidades no SIDA 33.8 % otras causas Weber R, Sabin CA, Friis-Moller N, Reis P, El-Sadr WM, Kirk O, et al. Liver-related deaths in persons infected with the human immunodeficiency virus: the D:A:D study. Arch Int Med 2006;166:
19 Smith CJ, Ryom L, Weber R, Morlat P, Pradier C, Reiss P, Kowalska JD, de Wit S, Law M, el Sadr W, Kirk O, Friis-Moller N, Monforte Ad, Phillips AN, Sabin CA, Lundgren JD. Trends in underlying causes of death in people with HIV from 1999 to 2011 (D: A: D): a multicohort collaboration. Lancet 2014; 384:

20 MAYOR MORTALIDAD POR INFECCIONES Entre 1997 y , pacientes VIH positivos con ESLD 15 (25,9%) fueron trasplantados, 21 (36,2%) murieron antes de OLTX, en promedio un mes luego de la de evaluación 57,1% por infección Ragni MV, Eghtesad B, Schlesinger KW, Dvorchik I, Fung JJ. Pretransplant survival is shorter in VIH-positive than VIHnegative subjects with end-stage liver disease. Liver Transpl 2005; 11:
21 INDICACION DE TRASPLANTE EN VIH CUANDO?
22 CRITERIOS ESPAÑOLES PARA TOH EN PACIENTES VIH Miró JM, Torre-Cisneros J, Moreno A et al. GESIDA/GESITRASEIMC, PNS and ONT consensus document on solid organ transplant (SOT) in VIH-infected patients in Spain March, Enferm Infecc Microbiol Clin, 2005, 23,
23 CRITERIOS ESPAÑOLES PARA TOH EN PACIENTES VIH Miró JM, Torre-Cisneros J, Moreno A et al. GESIDA/GESITRASEIMC, PNS and ONT consensus document on solid organ transplant (SOT) in VIH-infected patients in Spain March, Enferm Infecc Microbiol Clin, 2005, 23,
24 CRITERIOS ESPAÑOLES PARA TOH EN PACIENTES VIH Miró JM, Torre -Cisneros J, Moreno A et al. GESIDA/GESITRASEIMC, PNS and ONT consensus document on solid organ transplant (SOT) in VIH-infected patients in Spain March, Enferm Infecc Microbiol Clin, 2005, 23,
 in VIH-infected patients in Spain March, 2005.")
25 CRITERIOS ESPAÑOLES PARA TOH EN PACIENTES VIH Miró JM, Torre-Cisneros J, Moreno A et al. GESIDA/GESITRASEIMC, PNS and ONT consensus document on solid organ transplant (SOT) in VIH-infected patients in Spain March, Enferm Infecc Microbiol Clin, 2005, 23,
26 CRITERIOS EN EUROPA Y USA PARA TOH EN PACIENTES VIH Jose M. Miro, Peter Stock, Elina Teicher, Jean-Charles Duclos-Vallée, Norah Terrault, Antoni Rimola. Outcome and management of HCV/HIV coinfection pre- and post-liver transplantation. A 2015 update. Journal of Hepatology 2015 vol. 62,
27 CRITERIOS EN EUROPA Y USA PARA TOH EN PACIENTES VIH Jose M. Miro, Peter Stock, Elina Teicher, Jean-Charles Duclos-Vallée, Norah Terrault, Antoni Rimola. Outcome and management of HCV/HIV coinfection pre- and post-liver transplantation. A 2015 update. Journal of Hepatology 2015 vol. 62,
28 CRITERIOS EN EUROPA Y USA PARA TOH EN PACIENTES VIH Jose M. Miro, Peter Stock, Elina Teicher, Jean-Charles Duclos-Vallée, Norah Terrault, Antoni Rimola. Outcome and management of HCV/HIV coinfection pre- and post-liver transplantation. A 2015 update. Journal of Hepatology 2015 vol. 62,
29 CRITERIOS EN EUROPA Y USA PARA TOH EN PACIENTES VIH Jose M. Miro, Peter Stock, Elina Teicher, Jean-Charles Duclos-Vallée, Norah Terrault, Antoni Rimola. Outcome and management of HCV/HIV coinfection pre- and post-liver transplantation. A 2015 update. Journal of Hepatology 2015 vol. 62,
30 CRITERIOS EN EUROPA Y USA PARA TOH EN PACIENTES VIH Jose M. Miro, Peter Stock, Elina Teicher, Jean-Charles Duclos-Vallée, Norah Terrault, Antoni Rimola. Outcome and management of HCV/HIV coinfection pre- and post-liver transplantation. A 2015 update. Journal of Hepatology 2015 vol. 62,
31 TOH EN PACIENTES VIH - DESAFIOS ANTES DEL TOH Minimizar muertes en lista de espera, Remisiones tempranas. Evitar resistencia a drogas, no controlada. EN EL TOH Criterios expandidos de donantes Living donors, Excepciones al MELD en el futuro? Terrault NA, Carter JT, Carlson L, Roland ME, Stock PG. Outcome of patients with hepatitis B virus and human immunodeficiency virus infections referred for liver transplantation. Liver Transpl 2006;12: Ragni MV, Eghtesad B, Schlesinger KW, Dvorchik I, Fung JJ. Pretransplant survival is shorter in VIH-positive than VIHnegative subjects with end-stage liver disease. Liver Transpl 2005;11: Pineda JA, Romero-Gomez M, Diaz-Garcia F, Giron-Gonzalez JA, Montero JL, Torre-Cisneros J, et al. VIH coinfection shortens the survival of patients with hepatitis C virus-related decompensated cirrhosis. Hepatology 2005;41: Soriano V, Puoti M, Bonacini M, Brook G, Cargnel A, Rockstroh J, et al. Care of patients with chronic hepatitis B and VIH coinfection: recommendations from an VIH HBV International Panel. Aids 2005;19:
32 TOH EN PACIENTES VIH 2004 En la actualidad la infección por VIH ha dejado de ser una contraindicación formal para este tratamiento. Samuel D, Duclos Vallee JC, Teicher E, Vittecoq D. Liver transplantation in patients with VIH infection. J Hepatol, 2003, 39, 3 6. Roland ME, Stock PG. Review of solid-organ transplantation in VIH-infected patients. Transplantation, 2003, 75, Fung J, Eghtesad B, Patel-Tom K et al. Liver transplantation in patients with VIH infection. Liver Transpl, 2004, 10 (Suppl 2), S39 S53. Neff GW, Sherman KE, Eghtesad B, Fung J. Review article: current status of liver transplantation in VIHinfected patients. A l i m e n t Pharmacol Ther, 2004, 20, Miró JM, Montejo M, Rufi G et al. Liver transplantation in patients with VIH infection: a reality in Enferm Infecc Microbiol Clin, 2004, 22,
33 CONTRAINDICACIONES DEL TOH EN PACIENTES VIH Abuso de heroína o cocaína en los últimos dos años. Abuso de alcohol en los ultimos seis meses. IO activas o no controladas con la terapia ( leucoencefalopatía multifocal progresiva, criptosporidiasis intestinal crónica). Neoplasias para las que no se ha establecido un período libre de enfermedad adecuado. Síndrome de emaciación crónica. Desnutrición severa. Jose M. Miro, Peter Stock, Elina Teicher, Jean-Charles Duclos-Vallée, Norah Terrault, Antoni Rimola. Outcome and management of HCV/HIV coinfection pre- and post-liver transplantation. A 2015 update. Journal of Hepatology 2015 vol. 62,
34 RESULTADOS DEL TRASPLANTE (TOH)

35 Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
36 TOH EN COINFECCION VIH-VHC PRINCIPAL PROBLEMA POS-TOH ES LA SEVERIDAD DE LA RECURRENCIA DE LA INFECCION VHC EN EL INJERTO Duclos-Vallee JC, Feray C, Sebagh M, Teicher E, Roque-Afonso AM,Roche B, et al. Survival and recurrence of hepatitiscafter liver transplantation in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology 2008;47: Duclos-Valle e JC, Vittecoq D, Teicher E, Feray C, Roque-Afonso AM, Lombes A, et al. VHC viral recurrence and liver mitochondrial damage after liver transplantation in VIH VHC coinfected patients. J Hepatol 2005;42: De Vera ME, Dvorchik I, Tom K, Eghtesad B, Thai N, Shakil O, et al. Survival of liver transplant patients coinfected with VIH and VHC is adversely impacted by recurrent hepatitis C. Am J Transpl 2006;6:
37 RECURRENCIA DEL VIRUS C Recurrencia universal. Peor evolución. Eficacia y seguridad del tto con Peg- IFN mas Riba?? Ragni MV, Belle SH, Im K et al. Survival of human immunodeficiency virus-infected liver transplant recipients. J Infect Dis, 2003, 188, Duclos-Vallee JC, Vittecoq D, Teicher E et al. Hepatitis C virus viral recurrence and liver mitochondrial damage after liver transplantation in VIH-VHC co-infected patients. J Hepatol, 2005, 42, De Vera ME, Dvorchik I, Tom K et al. Survival of liver transplant patients co-infected with VIH and VHC is adversely impacted by recurrent hepatitis C. Am J Transplant, 2006, 6,
38 TOH EN PACIENTES VIH PRINCIPALES SERIES ANTES Y DESPUES DEL TARGA Miró et al. Journal of VIH therapy Vol 12 No Miró et al. Journal of VIH therapy Vol 12 No

39 TOH EN PACIENTES VIH PRINCIPALES SERIES ANTES Y DESPUES DEL TARGA Miró et al. Journal of VIH therapy Vol 12 No Miró et al. Journal of VIH therapy Vol 12 No
, C-103. 26.")
40 21. Fung J, Eghtesad B, Patel-Tom K et al. Liver transplantation in patients with VIH infection. Liver Transpl, 2004, 10 (Suppl 2), S39 S Duclos-Vallee JC, Teicher E, Feray C et al. Liver transplantation of VIH-VHC and VIH-HBV coinfected patients: a large experience in a single centre. Abstract number 410. Liver Transplant, 2006, 12(Suppl 1), C De Vera ME, Dvorchik I, Tom K et al. Survival of liver transplant patients co-infected with VIH and VHC is adversely impacted by recurrent hepatitis C. Am J Transplant, 2006, 6, Vennarecci G, Mutimer D, Ettorre G et al. Liver transplantation in VIH-positive patients. Abstract number 457. Liver Transplant, 2006, 12 (Suppl 1), C Castells L, Escartin A, Bilbao I et al. Liver transplantation in VIH-VHC coinfected patients: a case-control study. Transplantation, 2007, 83, Miró JM, Montejo M, Castells LL et al. Treatment of Spanish VIH-infected patients with recurrent hepatitis C virus (VHC) after liver transplantation (OLT) with pegylated interferon (PEG-INF) plus ribavirin (RBV): preliminary results of the FIPSE OLT-VIH-05 GESIDA Cohort Study ( ). 14th Conference on Retroviruses and Opportunistic Infections. Los Angeles, California, USA February 2007, Abstr. 890.



41 1. Duclos-Vallee JC, Feray C, Sebagh M, Teicher E, Roque-Afonso AM, Roche B, et al. Survival and recurrence of hepatitis C after liver transplantation in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology 2008;47: Miro JM, Montejo M, Castells L, Rafecas A, Moreno S, Aguero F, et al. Outcome of HCV/HIV-coinfected liver transplant recipients: a prospective and multicenter cohort study. Am J Transplant 2012;12: Terrault NA, Roland ME, Schiano T, Dove L, Wong MT, Poordad F, et al. Outcomes of liver transplant recipients with hepatitis C and human immunodeficiency virus coinfection. Liver Transpl 2012;18: Jose M. Miro, Peter Stock, Elina Teicher, Jean-Charles Duclos-Vallée, Norah Terrault, Antoni Rimola. Outcome and management of HCV/HIV coinfection pre- and postliver transplantation. A 2015 update. Journal of Hepatology 2015 vol. 62,
42 Duclos-Vallée, Samuel D. Survival and recurrence of hepatitis C after liver transplantation in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology 2008; 47:
43 Se examinaron los resultados entre 180 pacientes VIH + con TOH (Registro Científico de Receptores de Trasplante ). Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
44 Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
45 Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
46 Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
47 Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
48 Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
49 Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
50 Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
51 Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
52 Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
53 Resultados. los receptores VIH + tuvieron un riesgo de muerte 1,68 veces mayor y 1,70 veces mayor riesgo de pérdida del injerto. Independientemente de la época del trasplante, los receptores coinfectados de TOH tuvieron un mayor riesgo de muerte (ahr, 2,24) y pérdida del injerto (ahr, 2,07; en comparación con los receptores de TOH HCV +. Conclusiones. Los resultados entre los receptores VIH + monoinfectados han mejorado con el tiempo, sin embargo, entre los coinfectados HIV+ VHC+ los datos siguen siendo preocupantes y motivan futuros estudios de beneficio de supervivencia. Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:

54 Umberto Baccarani, Elda Righi, Gian Luigi Adani, Dario Lorenzin, Alberto Pasqualucci, Matteo Bassetti, Andrea Risaliti. Pros and cons of liver transplantation in human immunodeficiency virus infected recipients. World J Gastroenterol 2014 May 14; 20(18):
55
56 FUTURO CON LOS NUEVOS ANTIVIRALES
![EFICACIA DE 12 SEMANAS DE DAA EN DIFERENTES ESTUDIOS DE VHC GT1-4 REGIMEN /RVS Monoinfección VHC Coinfección VIH/VHC SMV + SOF 97 (112/115) [1] 92 (11/12) [2] LDV/SOF 99 (211/214) [3] 95 (143/150)](/docs-images/65/53725418/images/57-1.jpg "[4] DCV + SOF 100 (41/41) [5] 97 (98/101) [6] OBV/PTV/RTV + DSV + RBV 96 (455/473) [7] 94 (29/31) [8] EBR/GZR 95 (299/316) [9] 95 (207/218) [10] SOF/VEL 99 (618/624) [11] 95 (101/106) [12] 1.")
57 EFICACIA DE 12 SEMANAS DE DAA EN DIFERENTES ESTUDIOS DE VHC GT1-4 REGIMEN /RVS Monoinfección VHC Coinfección VIH/VHC SMV + SOF 97 (112/115) [1] 92 (11/12) [2] LDV/SOF 99 (211/214) [3] 95 (143/150) [4] DCV + SOF 100 (41/41) [5] 97 (98/101) [6] OBV/PTV/RTV + DSV + RBV 96 (455/473) [7] 94 (29/31) [8] EBR/GZR 95 (299/316) [9] 95 (207/218) [10] SOF/VEL 99 (618/624) [11] 95 (101/106) [12] 1. Kwo P, et al. EASL 2015 Abstract LB Del Bello DP, et al. AASLD Abstract Afdhal N, et al. N Engl J Med. 2014;370: Naggie S, et al. N Engl J Med. 2015;373: Sulkowski M, et al. N Engl J Med. 2014;370: Wyles D, et al. N Engl J Med. 2015;373: Feld JJ, et al. N Engl J Med. 2014;370: Sulkowski M, et al. JAMA. 2015;313: Zeuzem S, et al. Ann Intern Med. 2015;163: Rockstroh JK, et al. AASLD Abstract Feld JJ, et al. N Engl J Med. 2015;373: Bräu N, et al. AIDS Abstract WEAB0301.
58 CONCLUSIONES
59 SOBREVIDA DEL PACIENTE VIH (%) EVOLUCION DE LA SOBREVIDA EN EL TRASPLANTE HEPATICO DE PACIENTES VIH POSITIVOS 100 Nueva era de antivirales sofosbuvir Daclatasvir 80 Inhibidores de integrasa Inmunosupresion alta Baja expectativa de vida Infecciones Oportunistas TARGA TARGA Reconstitucion inmunologica Mejor expectativa de vida
60 CONCLUSIONES 1 El trasplante hepático es una alternativa terapéutica en los pacientes VIH con una enfermedad hepática terminal Es posible controlar la infección por VIH tras el trasplante con tratamiento antirretroviral. Las interacciones entre los inmunosupresores y los antirretrovirales son importantes y exigen la monitorización estrecha de los niveles plasmáticos de inmunosupresores.
61 CONCLUSIONES 2 No existe un mayor riesgo de infecciones oportunistas ni de tumores En TOH por una cirrosis por VHC, la recidiva de la infección es universal postrasplante. Los nuevos tratamientos significan un avance enorme y se alcanzan tasas de sobrevida sorprendentes.
62
63
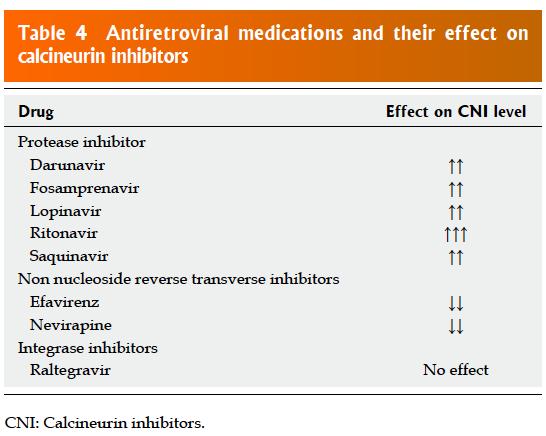
64 TRATAMIENTO ANTIRETROVIRAL Monitoreo estricto de la función hepática. Algunos medicamentos contraindicados en CH (Didanosina, Nevirapina, dosis plena de Ritonavir), se deben ajustar sus dosis según función hepática. Monitorizar niveles de Efavirenz e inhibidores de proteasa.???????? Indinavir y Atazanavir pueden incrementar bilirrubina no conjugada por inhibicion de UDPGT. Expert Committee of GESIDA and the National AIDS Plan. Recommendations from the GESIDA/Spanish AIDS Plan regarding antiretroviral treatment in adults with human immunodeficiency virus infection (Update January 2007). Enferm Infecc Microbiol Clin, 2007, 25, Wyles DL, Gerber J. Antiretroviral drug pharmacokinetics in hepatitis with hepatic dysfunction. Clin infect Dis, 2005, 40, Back D, Gibbons S. The University of Liverpool VIH drug interactions website: asp?pharmacology/pharma_main.asp [with access: 18/02/2007]. Tuset M, Miró JM, Codina C, Ribas J, Ed. Guía de interacciones en VIH: [with access: 18/02/200

65 CRITERIOS EN USA PARA TOH EN PACIENTES VIH En la Tabla 2 se enumeran las directrices de ensayos multicéntricos de los Estados Unidos para el trasplante hepático en pacientes VIH positivos con enfermedad hepática crónica.
66 Disminución significativa de la supervivencia del paciente VIH en la lista de espera y la importancia de la derivación temprana a esta evaluación. Stock PG. Rapid deterioration of VIH co-infected patients waiting for liver transplantation is not predicted by MELD. Liver Transpl 2005; 11:
 48 meses 74 61 44 VIH Positivos 180 (15%) 100 (56 %) 16 meses 54 40 25 RR de morir con IC de 95 % de 2.26 (1.51-3.38) 87 Pac TOH Pineda et. Al. Hepatology. 2005, 41, 779 789.")
67 N : 1217 pacientes con hepatitis C Seguimiento de 13 meses N Mortalid ad Sobrevi da Promedi o % Sobrevi da a 1 año % Sobrevi da a 2 años % Sobrevi da a 5 años % VIH Negativo s 1037 (85%) 386 (37 %) 48 meses VIH Positivos 180 (15%) 100 (56 %) 16 meses RR de morir con IC de 95 % de 2.26 ( ) 87 Pac TOH Pineda et. Al. Hepatology. 2005, 41,
68 AASLD Guidance: HIV/HCV Coinfection All pts with HCV should be treated Pts with cirrhosis among highest priority for treatment HIV/HCV coinfection among high priority for treatment Even in this era of potent HIV antiretrovirals, pts with HIV/HCV coinfection are at greater risk for rapidly progressive fibrosis and cirrhosis HIV ARV therapy is not a substitute for AASLD/IDSA. HCV guidelines. December Slide credit: clinicaloptions.com
69 DAAs for Pts With GT1 HCV Infection and HIV/HCV Coinfection No 8-wk regimens recommended in HIV/HCV coinfection Other recommendations on treatment duration and inclusion of RBV same as for HCV monoinfection HCV GT Recommended or Alternative Regimens for DAA-Naive Pts SMV + SOF LDV/SOF DCV + SOF OBV/PTV/ RTV + DSV EBR/GZR SOF/VEL Without cirrhosis 1a 12 wks 12 wks 12 wks 12 wks + RBV 12 wks 12 wks 1b 12 wks 12 wks 12 wks 12 wks 12 wks 12 wks With compensated cirrhosis 1a 24 wks ± RBV* 12 wks 24 wks ± RBV 24 wks + RBV 12 wks 12 wks 1b 24 wks ± RBV 12 wks 24 wks ± RBV 12 wks 12 wks 12 wks *Do not use if Q80K positive. If pegifn/rbv experienced, add RBV (recommended) or treat for 24 wks (alternative). If baseline NS5A RAVs, add RBV and treat for 16 wks (alternative). AASLD/IDSA. HCV guidance. July Slide credit: clinicaloptions.com
70 Efficacy of 12 Wks of DAAs Across Separate Studies of GT1- Sustained HCV Virologic Response, % (n/n) 4 HCV Infection HCV Monoinfection HIV/HCV Coinfection SMV + SOF 97 (112/115) [1] 92 (11/12) [2] LDV/SOF 99 (211/214) [3] 95 (143/150) [4] DCV + SOF 100 (41/41) [5] 97 (98/101) [6] OBV/PTV/RTV + DSV + RBV 96 (455/473) [7] 94 (29/31) [8] EBR/GZR 95 (299/316) [9] 95 (207/218) [10] SOF/VEL 99 (618/624) [11] 95 (101/106) [12] Most studies included HCV treatment-naive pts only, except for the SMV + SOF and SOF/VEL studies and the OBV/PTV/RTV + DSV + RBV coinfection study, which included both HCV treatment-naive and treatment-experienced pts Mostly GT1 and 4 HCV infection; some GT2, 3, 5, or 6 infection References in slidenotes. Slide credit: clinicaloptions.com
71

72 El trasplante hepático se realiza cada vez más en pacientes seleccionados con VIH en la mayoría de los países desarrollados, con excelentes resultados informados en pacientes con enfermedades hepáticas no relacionadas con el VHC. Por el contrario, la supervivencia en los receptores hepáticos coinfectados con el VHC / VIH es más pobre que en los pacientes monoinfectados con VHC, debido a la recurrencia más agresiva del VHC y la consecuente pérdida del injerto y la muerte. Los resultados de los estudios de cohortes estadounidenses, franceses y españoles mostraron una tasa de supervivencia de 5 años de sólo 50-55%. Por tanto, es Debatidó si el trasplante de hígado se debe ofrecer a los pacientes coinfectados con el VHC / VIH. Los estudios han demostrado que las variables más consistentemente asociadas con resultados pobres son: (1) el uso de donantes antiguos o HCV-positivos, (2) el trasplante de hígado-riñón dual, (3) receptores con un índice de masa corporal muy bajo y (4) menos experiencia en el sitio. Sin embargo, el factor más efectivo que influye en el resultado del trasplante es el éxito del tratamiento de la recurrencia del VHC con anti-vhc. La supervivencia es del 80% en pacientes cuya infección por VHC se resuelve. Lamentablemente, las tasas de respuesta virológica sostenida con interferón pegilado más ribavirina en receptores coinfectados son bajas, en particular para el genotipo 1 (sólo el 10%). Jose M. Miro, Peter Stock, Elina Teicher, Jean-Charles Duclos-Vallée, Norah Terrault, Antoni Rimola. Outcome and management of HCV/HIV coinfection pre- and post-liver transplantation. A 2015 update. Journal of Hepatology 2015 vol. 62,
73 ENFERMEDAD HEPATICA Y VIH Pineda JA, Romero-Gomez M, Diaz-Garcia F, Giron-Gonzalez JA, Montero JL, Torre-Cisneros J, et al. VIH coinfection shortens the survival of patients with hepatitis C virus-related decompensated cirrhosis. Hepatology 2005;41:
74 trasplante HEPATICO EN VIH Hasta hace unos años el VIH era una contraindicación absoluta para cualquier tipo de trasplante por: El pronóstico vital de estos pacientes y El temor a que la inmunosupresión asociada al trasplante pudiera acelerar la progresión a sida o incrementar el riesgo de infecciones oportunistas XXXXXXXXXXXXXXX
75 DAÑO HEPATICO AGUDO INDUCIDO POR TARGA (DILI) Infrecuente causa de severa morbilidad o mortalidad. Principalmente por Inhibidores de la Transcriptasa no nucleósidos En Nevirapina 3-15 % En Efavirenz 1-4 % de pacientes tratados con regímenes combinados. Sulkowski MS, Thomas DL, Chaisson RE, Moore RD. Hepatotoxicity associated with antiretroviral therapy in adults infected with human immunodeficiency virus and the role of hepatitis C or B virus infection. JAMA 2000;283: Nunez M. Hepatotoxicity of antiretrovirals: incidence, mechanisms and management. J Hepatol 2006;44:S132 S139.
76 DAÑO HEPATICO CRONICO INDUCIDO POR TARGA (DILI) 2 estudios observacionales(1-2) : 12 % y 9 % de incremento en la muertes de origen hepático por año de tto TARGA Enfermedad hepática criptogénica en 0.5 % de VIH, relacionados con TARGA?(3) [1] Weber R, Sabin CA, Friis-Moller N, Reis P, El-Sadr WM, Kirk O, et al. Liver-related deaths in persons infected with the human immunodeficiency virus: the D:A:D study. Arch Int Med 2006;166: [2] Mocroft A, Soriano V, Rockstroh J, Reiss P, Kirk O, De Wit S, et al. Is there evidence for an increase in the death rate from liverrelated disease in patients with VIH? Aids 2005;19: [3] Maida I, Nunez M, Rios MJ, Martin-Carbonero L, Sotgiu G, Toro C, et al. Severe liver disease associated with prolonged exposure to antiretroviral drugs. J Acquir Immune Defic Syndr 2006;42:

77 PACIENTES VIH CANDIDATOS A EVALUACION PRE-TOH 2005 Fung J, Eghtesad B, Patel-Tom K et al. Liver transplantation in patients with VIH infection. Liver Transpl, 2004, 10 (Suppl 2), S39 S53. Hamers FF, Downs AM. The changing face of the VIH epidemic in western Europe: what are the implications for public health policies? Lancet, 2004, 364, Rockstroh J, Mocroft A, Soriano V et al. Influence of hepatitis C coinfection on VIH disease Progression within the Eurosida cohort. 9th European AIDS Conference. Warsaw, Poland, October2003. Abstr. F12/4. Konopnicki D, Mocroft A, de Wit S et al. Hepatitis B and VIH: prevalence, AIDS progression, response to highly active antiretroviral therapy and increased mortality in the EuroSIDA cohort. AIDS, 2005, 19, Gonzalez-GarcÌa JJ, Mahillo B, Hern ndez S et al. Prevalences of hepatitis virus coinfection and indications for chronic hepatitis C virus treatment and liver transplantation in Spanish VIH-infected patients. The GESIDA 29/02 and FIPSE 12185/01 Multicenter Study. Enferm Infecc Microbiol Clin, 2005, 23,
 Duclos-Vallée, Samuel D. Survival and recurrence of hepatitis C after liver transplantation in patients coinfected with human immunodeficiency virus and hepatitis C virus.")
78 Fibrosis a los 12 meses después del trasplante puntuación media de 1,7 en pacientes coinfectados en comparación con 1,1 en pacientes monoinfectados (p = 0,06); A los 24 meses, 2,4 frente a 1,4, respectivamente (P = 0,01) Duclos-Vallée, Samuel D. Survival and recurrence of hepatitis C after liver transplantation in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology 2008; 47:
79 Se examinaron los resultados entre 180 pacientes VIH + con TOH (Registro Científico de Receptores de Trasplante ). Resultados. los receptores VIH + tuvieron un riesgo de muerte 1,68 veces mayor (HR ajustado, 1,68, intervalo de confianza del 95% [IC del 95%], 1,28-2,20, P <0,001) y 1,70 veces mayor riesgo de pérdida del injerto (HR, 1,70, IC del 95%, 1,31-2,20, P <0,001). Estas diferencias persistieron independientemente del estado de infección por VHC. Sin embargo, en el riesgo de muerte en la edad de trasplante (HR, 1,11, IC del 95%, 0,52-2,35, P = 0,79) y pérdida del injerto (ahr, 0,89, IC del 95%, 0,42-1,88, P = 0,77) fueron similares entre los monoinfectados y receptores de TOH no infectados. En contraste, independientemente de la época del trasplante, los receptores coinfectados de TOH tuvieron un mayor riesgo de muerte (ahr, 2,24, IC 95%, 1,43-3,53, P <0,001) y pérdida del injerto (ahr, 2,07; IC del 95%, 1,33-3,22; = 0,001) en comparación con los receptores de TOH HCV +. Conclusiones. Estos resultados sugieren que los resultados entre los receptores de VIH + monoinfectados han mejorado con el tiempo, sin embargo, los resultados entre los receptores de HIV + coinfectados con el VHC siguen siendo preocupantes y motivan futuros estudios de beneficio de supervivencia. Jayme E. Locke, Christine Durand, Rhiannon D. Reed, et al Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus Infected Recipients. Transplantation 2016; 100:
80 PERIODO POST-TOH No hay un riesgo aumentado de complicaciones POP. No hay mayor riesgo de infecciones oportunistas o tumores Con tratamiento TARGA adecuado CD4 estables. Carga viral VIH indetectable Medicamentos inmunosupresores( IC, CT,MMF) reducen la replicación viral por 2 vias Reduciendo activación inmune del VIH IC y MMF actividad antiviral directa Acido micofenolico aumenta actividad de Abacavir. Roland ME, Stock PG. Review of solid-organ transplantation in VIH-infected patients. Transplantation, 2003, 75, Fung J, Eghtesad B, Patel-Tom K et al. Liver transplantation in patients with VIH infection. Liver Transpl, 2004, 10 (Suppl 2), S39 S Neff GW, Sherman KE, Eghtesad B, Fung J. Review article: current status of liver transplantation in VIH-infected patients. A l i m e n t Pharmacol Ther, 2004, 20, Miró JM, Montejo M, Rufi G et al. Liver transplantation in patients with VIH infection: a reality in Enferm Infecc Microbiol Clin, 2004, 22, Tzakis AG, Coope Margolis, D, Kewn S, Coull JJ et al. The addition of mycophenolate mofetil to antiretroviral therapy including abacavir is associated with depletion of intracellular deoxyguanosine triphosphate and a decrease in plasma VIH-1 RNA. J Acquir Immune Defic Syndr, 2002, 31,
81 PERIODO POST-TOH Gran cantidad de medicamentos : Mejor adherencia Menor toxicidad Menos interacciones con otros medicamentos Mayor efectividad Monitoreo estricto de función hepática. Protocolos de manejo iguales a los pacientes no VIH. Miró, Rimola. et al. Journal of VIH therapy Vol 12 No

82 Umberto Baccarani, Elda Righi, Gian Luigi Adani, Dario Lorenzin, Alberto Pasqualucci, Matteo Bassetti, Andrea Risaliti. Pros and cons of liver transplantation in human immunodeficiency virus infected recipients. World J Gastroenterol 2014 May 14; 20(18):
Virus C y Hepatocarcinoma. Perspectivas en 2013
 Pamplona, junio de 2008 Virus C y Hepatocarcinoma. Perspectivas en 2013 Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Epidemiología del HCC en Europa Globalmente 50.000 casos nuevos
Pamplona, junio de 2008 Virus C y Hepatocarcinoma. Perspectivas en 2013 Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Epidemiología del HCC en Europa Globalmente 50.000 casos nuevos
Coinfección VIH / VHC Juan E. Losa Hospital U. F. Alcorcón. Universidad Rey Juan Carlos Madrid
 Coinfección VIH / VHC Juan E. Losa Hospital U. F. Alcorcón. Universidad Rey Juan Carlos Madrid Coinfección y Hepatitis víricas: Nuevas soluciones. Guión 1.- Nuevos tratamientos antivhc: un cambio en la
Coinfección VIH / VHC Juan E. Losa Hospital U. F. Alcorcón. Universidad Rey Juan Carlos Madrid Coinfección y Hepatitis víricas: Nuevas soluciones. Guión 1.- Nuevos tratamientos antivhc: un cambio en la
ESTRATEGIA TERAPÉUTICA PARA LA HEPATITIS CRÓNICA CAUSADA POR EL VIRUS DE LA HEPATITIS C EN EL SISTEMA NACIONAL DE SALUD
 ESTRATEGIA TERAPÉUTICA PARA LA HEPATITIS CRÓNICA CAUSADA POR EL VIRUS DE LA HEPATITIS C EN EL SISTEMA NACIONAL DE SALUD Recomendaciones generales y pautas actuales de tratamiento Plan Estratégico para
ESTRATEGIA TERAPÉUTICA PARA LA HEPATITIS CRÓNICA CAUSADA POR EL VIRUS DE LA HEPATITIS C EN EL SISTEMA NACIONAL DE SALUD Recomendaciones generales y pautas actuales de tratamiento Plan Estratégico para
VIH/SIDA, tratamiento antiretroviral
 VIH/SIDA, tratamiento antiretroviral Dr. Samuel Navarro Alvarez, MSP Medico Internista e Infectólogo Objetivos de aprendizaje Mostrar los beneficios del tratamiento anti retroviral Describir cuales son
VIH/SIDA, tratamiento antiretroviral Dr. Samuel Navarro Alvarez, MSP Medico Internista e Infectólogo Objetivos de aprendizaje Mostrar los beneficios del tratamiento anti retroviral Describir cuales son
TRASPLANTE HEPÁTICO EN VIH. Ana Belén Galera Rodenas MIR AP. DIGESTIVO
 TRASPLANTE HEPÁTICO EN VIH Ana Belén Galera Rodenas MIR AP. DIGESTIVO DOCUMENTO DE CONSENSO GESIDA/ GESITRA SEIMC, SPNS Y ONT SOBRE TRASPLANTE DE ÓRGANO SÓLIDO EN PACIENTES INFECTADOS POR EL VIH EN ESPAÑA
TRASPLANTE HEPÁTICO EN VIH Ana Belén Galera Rodenas MIR AP. DIGESTIVO DOCUMENTO DE CONSENSO GESIDA/ GESITRA SEIMC, SPNS Y ONT SOBRE TRASPLANTE DE ÓRGANO SÓLIDO EN PACIENTES INFECTADOS POR EL VIH EN ESPAÑA
BIBLIOGRAFÍA INTERNACIONAL
 BIBLIOGRAFÍA INTERNACIONAL Antiviral Therapy Predicted effect of direct acting antivirals in the current HIV HCV coinfected Predicción del efecto de los agentes antivirales de acción directa en la población
BIBLIOGRAFÍA INTERNACIONAL Antiviral Therapy Predicted effect of direct acting antivirals in the current HIV HCV coinfected Predicción del efecto de los agentes antivirales de acción directa en la población
350 millones de personas infectadas crónicamente 75% se encuentran en Asia y Pacífico 1 millón de muertes relacionadas a infección por HVB Representa
 350 millones de personas infectadas crónicamente 75% se encuentran en Asia y Pacífico 1 millón de muertes relacionadas a infección por HVB Representa el 5-10% de los trasplantes hepáticos La infección
350 millones de personas infectadas crónicamente 75% se encuentran en Asia y Pacífico 1 millón de muertes relacionadas a infección por HVB Representa el 5-10% de los trasplantes hepáticos La infección
Resultados de la cohorte Española de Trasplante Hepático en pacientes VIH (+): Análisis de los 116 casos en la era TARGA.
: Análisis de los 116 casos en la era TARGA.") Resultados de la cohorte Española de Trasplante Hepático en pacientes VIH (+): Análisis de los 116 casos en la era TARGA. Estudio FIPSE OLT-HIV-05 - GESIDA (2002-07) L. Castells 1, JR Fernández 2, JC Meneu
Resultados de la cohorte Española de Trasplante Hepático en pacientes VIH (+): Análisis de los 116 casos en la era TARGA. Estudio FIPSE OLT-HIV-05 - GESIDA (2002-07) L. Castells 1, JR Fernández 2, JC Meneu
Eficacia y Seguridad de la Triple Terapia en HCU. Estado Actual Tratamiento VHC. Guillermo García Rayado MIR 3º Año. Digestivo
 Eficacia y Seguridad de la Triple Terapia en HCU Estado Actual Tratamiento VHC Guillermo García Rayado MIR 3º Año. Digestivo Eficacia y Seguridad de la Triple Terapia en Pacientes con Hepatitis Crónica
Eficacia y Seguridad de la Triple Terapia en HCU Estado Actual Tratamiento VHC Guillermo García Rayado MIR 3º Año. Digestivo Eficacia y Seguridad de la Triple Terapia en Pacientes con Hepatitis Crónica
Controversias en hepatitis Viral II
 Controversias en hepatitis Viral II Dra. Ángeles Castro Iglesias Servicio de Medicina Interna B Hospital Universitario de A Coruña VI Curso de Biología Molecular para Clínicos Vigo, 3-4 de Febrero de 2012
Controversias en hepatitis Viral II Dra. Ángeles Castro Iglesias Servicio de Medicina Interna B Hospital Universitario de A Coruña VI Curso de Biología Molecular para Clínicos Vigo, 3-4 de Febrero de 2012
TRATAMIENTO ANTIVIRAL DE LA CIRROSIS HEPÁTICA POR VIRUS DE LA HEPATITIS B Y C
 TRATAMIENTO ANTIVIRAL DE LA CIRROSIS HEPÁTICA POR VIRUS DE LA HEPATITIS B Y C Dra. Ángeles Castro Servicio de Medicina Interna B Hospital Universitario de A Coruña Vigo, 15 de Enero de 2010 Progresión
TRATAMIENTO ANTIVIRAL DE LA CIRROSIS HEPÁTICA POR VIRUS DE LA HEPATITIS B Y C Dra. Ángeles Castro Servicio de Medicina Interna B Hospital Universitario de A Coruña Vigo, 15 de Enero de 2010 Progresión
Efectos Secundarios Telaprevir Boceprevir. Anemia 32% 49% Neutropenia 5 % grado 3-4 29 % grado 3-4. Molestias anorrectales 27 % - Rash 55 % 15-18 %
 FARMACOTERAPIA Manejo del tratamiento de la Hepatitis C Crónica Genotipo 1 María Pérez Abánades 1 y Concepción Martínez Nieto 1 La infección por el virus de la hepatitis C (VHC) es un problema de salud
FARMACOTERAPIA Manejo del tratamiento de la Hepatitis C Crónica Genotipo 1 María Pérez Abánades 1 y Concepción Martínez Nieto 1 La infección por el virus de la hepatitis C (VHC) es un problema de salud
Relación entre diabetes y VHC antes y después del transplante hepático
 Relación entre diabetes y VHC antes y después del transplante hepático Dr Xavier Xiol Hospital Universitari de Bellvitge L Hospitalet de Llobregat Barcelona Definiciones Diabetes tipo 1 Secundaria déficit
Relación entre diabetes y VHC antes y después del transplante hepático Dr Xavier Xiol Hospital Universitari de Bellvitge L Hospitalet de Llobregat Barcelona Definiciones Diabetes tipo 1 Secundaria déficit
Hospital Universitari Vall Hebron. Barcelona
 ELEVADA EFICACIA Y SEGURIDAD DEL TRATAMIENTO CON SOFOSBUVIR Y DACLATASVIR EN EL TRATAMIENTO DE LA RECIDIVA POR VHC POST-TRASPLANTE TANTO EN PACIENTES MONO COMO COINFECTADOS POR VIH J. Llaneras (1,2), I.
ELEVADA EFICACIA Y SEGURIDAD DEL TRATAMIENTO CON SOFOSBUVIR Y DACLATASVIR EN EL TRATAMIENTO DE LA RECIDIVA POR VHC POST-TRASPLANTE TANTO EN PACIENTES MONO COMO COINFECTADOS POR VIH J. Llaneras (1,2), I.
Grupo de Estudio de Hepatitis. GEHEP Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica SOLICITUD DE PROYECTO DE INVESTIGACION
 SOLICITUD DE PROYECTO DE INVESTIGACION 1. Datos del proyecto Título del proyecto: Eficacia y seguridad del tratamiento con Simeprevir para Hepatitis crónica C genotipo 4 en la práctica clínica habitual.
SOLICITUD DE PROYECTO DE INVESTIGACION 1. Datos del proyecto Título del proyecto: Eficacia y seguridad del tratamiento con Simeprevir para Hepatitis crónica C genotipo 4 en la práctica clínica habitual.
Terapia Virus Hepatitis C en pacientes cirróticos Dr Francisco Fuster S. Hospital G Fricke Viña del Mar
 Terapia Virus Hepatitis C en pacientes cirróticos 2015 Dr Francisco Fuster S. Hospital G Fricke Viña del Mar Conflictos de interés Charlas, ayuda para proyectos de investigación o reuniones de consejería
Terapia Virus Hepatitis C en pacientes cirróticos 2015 Dr Francisco Fuster S. Hospital G Fricke Viña del Mar Conflictos de interés Charlas, ayuda para proyectos de investigación o reuniones de consejería
Ignacio de los Santos Gil Hospital Universitario de la Princesa Madrid
 Ignacio de los Santos Gil Hospital Universitario de la Princesa Madrid OMS Guidelines for the screening and treatment of persons with hepatitis C infection. April 2014 2 Infección VIH y VHC: grave problema
Ignacio de los Santos Gil Hospital Universitario de la Princesa Madrid OMS Guidelines for the screening and treatment of persons with hepatitis C infection. April 2014 2 Infección VIH y VHC: grave problema
HEPATITIS C RECURRENTE DESPUÉS DEL TRASPLANTE HEPÁTICO
 477 47 HEPATITIS C RECURRENTE DESPUÉS DEL TRASPLANTE HEPÁTICO M Berenguer M Prieto La cirrosis secundaria a la infección crónica por el virus de la hepatitis C (VHC) es la principal indicación de trasplante
477 47 HEPATITIS C RECURRENTE DESPUÉS DEL TRASPLANTE HEPÁTICO M Berenguer M Prieto La cirrosis secundaria a la infección crónica por el virus de la hepatitis C (VHC) es la principal indicación de trasplante
TOLERANCIA A LA TRIPLE TERAPIA EN POBLACIONES ESPECIALES
 TOLERANCIA A LA TRIPLE TERAPIA EN POBLACIONES ESPECIALES C a r m e n V i n a i x a, C a r l a S a t o r r e s, B e a t r i z R o d r í g u e z, M a r í a G a r c í a, V i c t o r i a A g u i l e r a, A
TOLERANCIA A LA TRIPLE TERAPIA EN POBLACIONES ESPECIALES C a r m e n V i n a i x a, C a r l a S a t o r r e s, B e a t r i z R o d r í g u e z, M a r í a G a r c í a, V i c t o r i a A g u i l e r a, A
Coinfección VIH / VHC /VHB. Aspectos relevantes de su seguimiento.
 Coinfección VIH / VHC /VHB. Aspectos relevantes de su seguimiento. VIH VHC VHB Porque es importante tener en cuenta la coinfección por VHC y por VHB en el paciente VIH? Importancia epidemiológica 1ª) Alta
Coinfección VIH / VHC /VHB. Aspectos relevantes de su seguimiento. VIH VHC VHB Porque es importante tener en cuenta la coinfección por VHC y por VHB en el paciente VIH? Importancia epidemiológica 1ª) Alta
trasplante hepático y la recidiva de la hepatitis C en el embargo, la historia natural de la recidiva de la hepatitis C es
 Evoluciones atípicas de la recidiva de la hepatitis C en el trasplante hepático. Dra. Teresa Serrano. Hospital de Bellvitge. Barcelona. La cirrosis por hepatitis C es la principal indicación de trasplante
Evoluciones atípicas de la recidiva de la hepatitis C en el trasplante hepático. Dra. Teresa Serrano. Hospital de Bellvitge. Barcelona. La cirrosis por hepatitis C es la principal indicación de trasplante
2. La coinfección por el VIH acelera la progresión de la hepatitis crónica C y/o B.
 CONSECUENCIAS A LARGO PLAZO DE LA HEPATITIS C Y B EN DROGADICTOS INTRAVENOSOS INFECTADOS POR EL VIH Investigadores principales: Dr. Robert Muga Bustamante Hospital Universitari Germans Trias i Pujol Dr.
CONSECUENCIAS A LARGO PLAZO DE LA HEPATITIS C Y B EN DROGADICTOS INTRAVENOSOS INFECTADOS POR EL VIH Investigadores principales: Dr. Robert Muga Bustamante Hospital Universitari Germans Trias i Pujol Dr.
Coinfección por el VIH y el virus de la hepatitis C
 Servicio de Enfermedades Infecciosas. Hospital Carlos III. Madrid. España. Puntos clave Un tercio de los pacientes con infección por el VIH están coinfectados por el virus de la hepatitis C (VHC). Entre
Servicio de Enfermedades Infecciosas. Hospital Carlos III. Madrid. España. Puntos clave Un tercio de los pacientes con infección por el VIH están coinfectados por el virus de la hepatitis C (VHC). Entre
HEPATITIS B. Dra Silvia Borzi Servicio de Gastroenterología H.I.G.A. Prof. Dr. R. Rossi, La Plata
 HEPATITIS B Dra Silvia Borzi Servicio de Gastroenterología H.I.G.A. Prof. Dr. R. Rossi, La Plata Hepatitis B HBV : es un DNA virus que pertenece a la flia. Hepadnaviridae. Tiene forma redondeada con una
HEPATITIS B Dra Silvia Borzi Servicio de Gastroenterología H.I.G.A. Prof. Dr. R. Rossi, La Plata Hepatitis B HBV : es un DNA virus que pertenece a la flia. Hepadnaviridae. Tiene forma redondeada con una
FARMACOTERAPIA DE LA COINFECCIÓN VIH/VHC
 CASOS CLINICOS FARMACOTERAPIA DE LA COINFECCIÓN VIH/VHC Dra. Leonor Santos Morín Hospital Universitario Insular de G. C. Las Palmas de G.C Dra. Lourdes García Reina Hospital Universitario Insular de G.
CASOS CLINICOS FARMACOTERAPIA DE LA COINFECCIÓN VIH/VHC Dra. Leonor Santos Morín Hospital Universitario Insular de G. C. Las Palmas de G.C Dra. Lourdes García Reina Hospital Universitario Insular de G.
TRATAMIENTO DE LA INFECCION POR VHC Y CIRROIS
 TRATAMIENTO DE LA INFECCION POR VHC Y CIRROIS Juan González García. Jefe Sección Enfermedades Infecciosas Coordinador de Unidad VIH Hospital Universitario La Paz / IdiPAZ Conflictos de interés Juan González
TRATAMIENTO DE LA INFECCION POR VHC Y CIRROIS Juan González García. Jefe Sección Enfermedades Infecciosas Coordinador de Unidad VIH Hospital Universitario La Paz / IdiPAZ Conflictos de interés Juan González
HISTORIA NATURAL DE LA INFECCIÓN CRÓNICA POR EL VHC. Javier Murillas Medicina Interna Infecciosas Hospital Son Espases Palma de Mallorca
 HISTORIA NATURAL DE LA INFECCIÓN CRÓNICA POR EL VHC Javier Murillas Medicina Interna Infecciosas Hospital Son Espases Palma de Mallorca Por qué tenemos que hablar de historia natural? Limitaciones de los
HISTORIA NATURAL DE LA INFECCIÓN CRÓNICA POR EL VHC Javier Murillas Medicina Interna Infecciosas Hospital Son Espases Palma de Mallorca Por qué tenemos que hablar de historia natural? Limitaciones de los
Resultados de la práctica clínica en. Miguel A von Wichmann
 Resultados de la práctica clínica en la coinfección ió VIH/VHC Miguel A von Wichmann Hosp Univ Donostia, San Sebastián RVS con AAD en pacientes coinfectados Gt-1 sin tratamiento previo (EC) TVR BOC Distribución
Resultados de la práctica clínica en la coinfección ió VIH/VHC Miguel A von Wichmann Hosp Univ Donostia, San Sebastián RVS con AAD en pacientes coinfectados Gt-1 sin tratamiento previo (EC) TVR BOC Distribución
Tratamiento Antirretroviral y Perspectivas de Futuro. Juan E. Losa. 18 de junio de 2009 18:45-19:45
 Tratamiento Antirretroviral y Perspectivas de Futuro Juan E. Losa 18 de junio de 2009 18:45-19:45 TAR y Perspectivas de Futuro Guión 1.- Lo básico 2.- El rollo 3.- Lo interesante 4.- Lo necesario 5.-
Tratamiento Antirretroviral y Perspectivas de Futuro Juan E. Losa 18 de junio de 2009 18:45-19:45 TAR y Perspectivas de Futuro Guión 1.- Lo básico 2.- El rollo 3.- Lo interesante 4.- Lo necesario 5.-
Hospital General Universitario Valle Hebron
 TRATAMIENTO DE LA S HEPATITIS VIRALES Maria Buti. Servicio de Hepatología- Medicina Interna Hospital General Universitario Valle de Hebrón. Barcelona. Dirección. Dra Maria Buti Servicio de Hepatología
TRATAMIENTO DE LA S HEPATITIS VIRALES Maria Buti. Servicio de Hepatología- Medicina Interna Hospital General Universitario Valle de Hebrón. Barcelona. Dirección. Dra Maria Buti Servicio de Hepatología
SITUACIÓN ACTUAL Y MANEJO DEL VIH-SIDA
 SITUACIÓN ACTUAL Y MANEJO DEL VIH-SIDA Augusto G. Escalante Candia Médico Infectólogo Hospital Regional Docente de Medicina Tropical Pedro Ortiz Cabanillas VIH SIDA: OMS 2014 35 millones de personas
SITUACIÓN ACTUAL Y MANEJO DEL VIH-SIDA Augusto G. Escalante Candia Médico Infectólogo Hospital Regional Docente de Medicina Tropical Pedro Ortiz Cabanillas VIH SIDA: OMS 2014 35 millones de personas
Adolescentes con infección VIH: Adherencia
 Adolescentes con infección VIH: Adherencia Dra. Solange Arazi Caillaud Infectóloga pediatra Médica especialista del Servicio de Control Epidemiológico e Infectología Hospital de Pediatría J.P. Garrahan
Adolescentes con infección VIH: Adherencia Dra. Solange Arazi Caillaud Infectóloga pediatra Médica especialista del Servicio de Control Epidemiológico e Infectología Hospital de Pediatría J.P. Garrahan
Dr. Rodolfo Pinzón Meza Clínica de Enfermedades Infecciosas Hospital Roosevelt LA TERAPIA ANTIRRETROVIRAL Y TUBERCULOSIS.
 Dr. Rodolfo Pinzón Meza Clínica de Enfermedades Infecciosas Hospital Roosevelt LA TERAPIA ANTIRRETROVIRAL Y TUBERCULOSIS. COINFECCION TB/VIH Cuando creíamos que la batalla frente a la Tuberculosis se
Dr. Rodolfo Pinzón Meza Clínica de Enfermedades Infecciosas Hospital Roosevelt LA TERAPIA ANTIRRETROVIRAL Y TUBERCULOSIS. COINFECCION TB/VIH Cuando creíamos que la batalla frente a la Tuberculosis se
Artículo original. Manuel Manzano Luque, Médico, Hospital Universitario de la Princesa, Madrid, España
 Artículo original Salud(i)Ciencia 20 (2014) 357-361 Características de una población coinfectada por el VIH y los virus de las hepatitis B y C por medio de los resultados de la elastografía de transición
Artículo original Salud(i)Ciencia 20 (2014) 357-361 Características de una población coinfectada por el VIH y los virus de las hepatitis B y C por medio de los resultados de la elastografía de transición
Es frecuente la infección crónica por el virus de hepatitis B (VHB)?
?") HEPATITIS B Qué es la hepatitis B y tipos? La hepatitis B es una enfermedad producida por la infección de un virus de tipo ADN, que infecta e inflama el hígado. Puede producir un cuadro agudo (hepatitis
HEPATITIS B Qué es la hepatitis B y tipos? La hepatitis B es una enfermedad producida por la infección de un virus de tipo ADN, que infecta e inflama el hígado. Puede producir un cuadro agudo (hepatitis
Análisis de la coestimulación vía CD28 en células linfoides de pacientes infectados. con el virus de la Hepatitis C RESUMEN
 Análisis de la coestimulación vía CD28 en células linfoides de pacientes infectados con el virus de la Hepatitis C RESUMEN La infección por el virus de la hepatitis C (VHC) afecta a más de 170 millones
Análisis de la coestimulación vía CD28 en células linfoides de pacientes infectados con el virus de la Hepatitis C RESUMEN La infección por el virus de la hepatitis C (VHC) afecta a más de 170 millones
Boletín de la SEICV, nueva época
 Boletín de la Sociedad de Enfermedades Infecciosas de la Comunidad Valenciana VOLUMEN 2 NÚMER O 1 MAYO 2013 En este número: 1. Presentación nueva época 2. Resúmenes del 48th Annual Meeting of the European
Boletín de la Sociedad de Enfermedades Infecciosas de la Comunidad Valenciana VOLUMEN 2 NÚMER O 1 MAYO 2013 En este número: 1. Presentación nueva época 2. Resúmenes del 48th Annual Meeting of the European
Atención y tratamiento en VIH/sida Parte 1
 UNIVERSIDAD NACIONAL AUTONOMA DE NICARAGUA CENTRO DE INVESTIGACIONES Y ESTUDIOS DE LA SALUD DIPLOMADO CENTROAMERICANO SOBRE MONITOREO Y EVALUACIÓN DE POLÍTICAS Y PROGRAMAS DE VIH-SIDA Atención y tratamiento
UNIVERSIDAD NACIONAL AUTONOMA DE NICARAGUA CENTRO DE INVESTIGACIONES Y ESTUDIOS DE LA SALUD DIPLOMADO CENTROAMERICANO SOBRE MONITOREO Y EVALUACIÓN DE POLÍTICAS Y PROGRAMAS DE VIH-SIDA Atención y tratamiento
Hepatitis C al 2014: Tractar o esperar ALTRES GENOTIPS (NO 1)
") Hepatitis C al 2014: Tractar o esperar ALTRES GENOTIPS (NO 1) XXIII Congrés de la Societat Catalana de Digestologia 31 de gener, Palau de Congressos de Lleida.La Llotja Dr. Joan Carles Quer Htal. Universitari
Hepatitis C al 2014: Tractar o esperar ALTRES GENOTIPS (NO 1) XXIII Congrés de la Societat Catalana de Digestologia 31 de gener, Palau de Congressos de Lleida.La Llotja Dr. Joan Carles Quer Htal. Universitari
BIBLIOGRAFÍA COMENTADA
 BIBLIOGRAFÍA COMENTADA GUT HCV substitutions and IL-28B polymorphisms on outcome of peg-interferon plus ribavirin combination therapy Efecto de las variantes del VHC y los polimorfismos del gen IL-28B
BIBLIOGRAFÍA COMENTADA GUT HCV substitutions and IL-28B polymorphisms on outcome of peg-interferon plus ribavirin combination therapy Efecto de las variantes del VHC y los polimorfismos del gen IL-28B
III CONGRESO NACIONAL DE ATENCIÓN FARMACÉUTICA
 Adherencia a la terapia antirretroviral en pacientes infectados con el virus de la inmunodeficiencia humana que asisten a una clínica universitaria de enfermedades infecciosas en Venezuela. III CONGRESO
Adherencia a la terapia antirretroviral en pacientes infectados con el virus de la inmunodeficiencia humana que asisten a una clínica universitaria de enfermedades infecciosas en Venezuela. III CONGRESO
ESQUEMAS DE TRATAMIENTO
 V. Tratamiento C. Esquemas de tratamiento Óscar Beltrán Galvis MD, 1 Mónica Tapias, MD, 2 Víctor Idrovo, MD. 3 1 Internista, Gastroenterólogo y Hepatólogo. UIS y Universidad Nacional de Colombia. Grupo
V. Tratamiento C. Esquemas de tratamiento Óscar Beltrán Galvis MD, 1 Mónica Tapias, MD, 2 Víctor Idrovo, MD. 3 1 Internista, Gastroenterólogo y Hepatólogo. UIS y Universidad Nacional de Colombia. Grupo
Hepatitis C y los nuevos antivirales orales
 Sant Hilari de Sacalm, Hepatitis C y los nuevos antivirales orales Zoe Mariño, PhD, MD Hepatología. Hospital Clinic Barcelona 1 Agenda 1) Virus de la Hepatitis C (HCV). Prevalencia e historia natural.
Sant Hilari de Sacalm, Hepatitis C y los nuevos antivirales orales Zoe Mariño, PhD, MD Hepatología. Hospital Clinic Barcelona 1 Agenda 1) Virus de la Hepatitis C (HCV). Prevalencia e historia natural.
Sesión 1 - Inicio de TARV Coordinadores: Cristina Freuler Ricardo Marino- Celia Wainstein
 Sesión 1 - Inicio de TARV Coordinadores: Cristina Freuler Ricardo Marino- Celia Wainstein 5 - Inicio de TARV en situaciones especiales I a) co-infección con HVB/HVC b) con TBC Dra. Liliana Calanni, Dr.
Sesión 1 - Inicio de TARV Coordinadores: Cristina Freuler Ricardo Marino- Celia Wainstein 5 - Inicio de TARV en situaciones especiales I a) co-infección con HVB/HVC b) con TBC Dra. Liliana Calanni, Dr.
Insuficiencia Cardiaca. Betabloqueantes vs. Ivabradina. A favor de Ivabradina. Afonso Barroso de Freitas Ferraz
 Insuficiencia Cardiaca. Betabloqueantes vs. Ivabradina. A favor de Ivabradina Afonso Barroso de Freitas Ferraz Índice La FC en las enfermedades CV Betabloqueantes en IC Mecanismo de acción de la ivabradina
Insuficiencia Cardiaca. Betabloqueantes vs. Ivabradina. A favor de Ivabradina Afonso Barroso de Freitas Ferraz Índice La FC en las enfermedades CV Betabloqueantes en IC Mecanismo de acción de la ivabradina
DIRECCION DE SERVICIOS SANITARIOS
 PRODUCTOS SANITARIOS Página 1 de 5 Introducción La infección por el virus de la hepatitis C (VHC) es un problema de salud de primera magnitud en Europa y especialmente en los países mediterráneos, donde
PRODUCTOS SANITARIOS Página 1 de 5 Introducción La infección por el virus de la hepatitis C (VHC) es un problema de salud de primera magnitud en Europa y especialmente en los países mediterráneos, donde
Systematic review: Evaluation of adherence among treatment naïve patients with hepatitis C
 ARTÍCULO DE REVISIÓN Revisión sistemática: Evaluación de la adherencia del tratamiento de pacientes Systematic review: Evaluation of adherence among treatment naïve patients with hepatitis C 1 Servicio
ARTÍCULO DE REVISIÓN Revisión sistemática: Evaluación de la adherencia del tratamiento de pacientes Systematic review: Evaluation of adherence among treatment naïve patients with hepatitis C 1 Servicio
BIBLIOGRAFÍA INTERNACIONAL
 BIBLIOGRAFÍA INTERNACIONAL Clinical infectious diseases HIV infection is associated with decreased thrombin generation La infección por VIH se asocia con disminución de la generación de trombina Hsue PY
BIBLIOGRAFÍA INTERNACIONAL Clinical infectious diseases HIV infection is associated with decreased thrombin generation La infección por VIH se asocia con disminución de la generación de trombina Hsue PY
BIBLIOGRAFÍA COMENTADA
 BIBLIOGRAFÍA COMENTADA American Journal of Transplantation Donor and recipient IL-28B polymorphisms in HCV-infected patients undergoing antiviral therapy before and after liver transplantation Polimorfismos
BIBLIOGRAFÍA COMENTADA American Journal of Transplantation Donor and recipient IL-28B polymorphisms in HCV-infected patients undergoing antiviral therapy before and after liver transplantation Polimorfismos
HIPOGAMMAGLOBULINEMIA Y RIESGO DE INFECCIÓN EN RECEPTORES DE TRASPLANTE RENAL: resultados del estudio ATALANTA
 Barcelona, 18 de Marzo de 2011 The ATALANTA Study HIPOGAMMAGLOBULINEMIA Y RIESGO DE INFECCIÓN EN RECEPTORES DE TRASPLANTE RENAL: resultados del estudio ATALANTA Mario FERNÁNDEZ RUIZ a, Francisco LÓPEZ
Barcelona, 18 de Marzo de 2011 The ATALANTA Study HIPOGAMMAGLOBULINEMIA Y RIESGO DE INFECCIÓN EN RECEPTORES DE TRASPLANTE RENAL: resultados del estudio ATALANTA Mario FERNÁNDEZ RUIZ a, Francisco LÓPEZ
Inicio de la terapia antirretroviral: Cúal es el límite de CD4+ recomendado?
 Inicio de la terapia antirretroviral: Cúal es el límite de CD4+ recomendado? Adaptado de Clinical Care Options www.clinicaloptions.com por la Fundación Apoyarte DHHS 2009: Cuando empezar Recuento de CD4+
Inicio de la terapia antirretroviral: Cúal es el límite de CD4+ recomendado? Adaptado de Clinical Care Options www.clinicaloptions.com por la Fundación Apoyarte DHHS 2009: Cuando empezar Recuento de CD4+
Juan José Ros y Juan González García. Servicio Medicina Interna. Hospital La Paz. Madrid
 INFECCIÓN POR EL VIRUS DE LA HEPATITIS C EN PACIENTES INFECTADOS POR EL VIRUS DE LA INMUNODEFICIENCIA HUMANA: CARACTERÍSTICAS Y ASPECTOS DE SU EPIDEMIOLOGÍA, DIAGNÓSTICO Y TRATAMIENTO Juan José Ros y Juan
INFECCIÓN POR EL VIRUS DE LA HEPATITIS C EN PACIENTES INFECTADOS POR EL VIRUS DE LA INMUNODEFICIENCIA HUMANA: CARACTERÍSTICAS Y ASPECTOS DE SU EPIDEMIOLOGÍA, DIAGNÓSTICO Y TRATAMIENTO Juan José Ros y Juan
Informe Breve. Interferon Pegilado alfa 2 a y alfa 2b
 Informe Breve Interferon Pegilado alfa 2 a y alfa 2b Enero 2009 El día 16 de enero de 2009, el Area de Evaluación de Tecnologías en Salud de la Comisión Nacional Salud, Ciencia y Tecnologìa recibió una
Informe Breve Interferon Pegilado alfa 2 a y alfa 2b Enero 2009 El día 16 de enero de 2009, el Area de Evaluación de Tecnologías en Salud de la Comisión Nacional Salud, Ciencia y Tecnologìa recibió una
BIBLIOGRAFÍA INTERNACIONAL
 BIBLIOGRAFÍA INTERNACIONAL Antiviral Therapy Post exposure prophylaxis for HIV infection: a clinical trial comparing lopinavir/ritonavir versus atazanavir each with zidovudine/lamivudine Profilaxis postexposición
BIBLIOGRAFÍA INTERNACIONAL Antiviral Therapy Post exposure prophylaxis for HIV infection: a clinical trial comparing lopinavir/ritonavir versus atazanavir each with zidovudine/lamivudine Profilaxis postexposición
BIBLIOGRAFÍA INTERNACIONAL
 BIBLIOGRAFÍA INTERNACIONAL Clinical infectious diseases HIV-infected Ugandan adults taking antiretroviral therapy with CD4 counts > 200 cel/µl who discontinue cotrimoxazole prophylaxis have increased risk
BIBLIOGRAFÍA INTERNACIONAL Clinical infectious diseases HIV-infected Ugandan adults taking antiretroviral therapy with CD4 counts > 200 cel/µl who discontinue cotrimoxazole prophylaxis have increased risk
LA HEPATITIS C EN EL MEDIO PENITENCIARIO
 LA HEPATITIS C EN EL MEDIO PENITENCIARIO Como mejorar el acceso al tratamiento Pablo Saiz de la Hoya Zamácola Servicios Médicos. CP. Fontcalent. Alicante Coordinador GEISESP Prison Population HIV Prevalence
LA HEPATITIS C EN EL MEDIO PENITENCIARIO Como mejorar el acceso al tratamiento Pablo Saiz de la Hoya Zamácola Servicios Médicos. CP. Fontcalent. Alicante Coordinador GEISESP Prison Population HIV Prevalence
AUTORIDADES. Jesús Mantilla. Ministro del Poder Popular para la Salud. Dra. Nancy Pérez. Vice Ministra de Salud Colectiva.
 AUTORIDADES Jesús Mantilla. Ministro del Poder Popular para la Salud. Dra. Nancy Pérez. Vice Ministra de Salud Colectiva. Dra. Aleida Rivas. Directora General de Programas de Salud. Dra. Deisy Matos. Coordinadora
AUTORIDADES Jesús Mantilla. Ministro del Poder Popular para la Salud. Dra. Nancy Pérez. Vice Ministra de Salud Colectiva. Dra. Aleida Rivas. Directora General de Programas de Salud. Dra. Deisy Matos. Coordinadora
HEPATITIS CRÓNICA HOSPITAL DE LEÓN SERVICIO DE MEDICINA INTERNA. Diagnóstico. Laura Rodríguez Martín R1 Aparato Digestivo
 HEPATITIS CRÓNICA Diagnóstico Laura Rodríguez Martín R1 Aparato Digestivo DEFINICIÓN Proceso inflamatorio difuso en el hígado > 6 meses de evolución Criterios anatomopatológico: biopsia hepática D SP E
HEPATITIS CRÓNICA Diagnóstico Laura Rodríguez Martín R1 Aparato Digestivo DEFINICIÓN Proceso inflamatorio difuso en el hígado > 6 meses de evolución Criterios anatomopatológico: biopsia hepática D SP E
Carga viral y subpoblaciones linfocitarias en la infección con VIH- 1. Comparación entre sus determinaciones basales
 Revista Mexicana de Patología Clínica 1998; Volumen 45(3): 159-161 Carga viral y subpoblaciones linfocitarias en la infección con VIH- 1. Comparación entre sus determinaciones basales NOHEMI PATRICIA CASTILLO
Revista Mexicana de Patología Clínica 1998; Volumen 45(3): 159-161 Carga viral y subpoblaciones linfocitarias en la infección con VIH- 1. Comparación entre sus determinaciones basales NOHEMI PATRICIA CASTILLO
III Jornada Alcohol y Alcoholismo SEMI. Madrid, 26 Abril 2014
 III Jornada Alcohol y Alcoholismo SEMI Madrid, 26 Abril 2014 Estudio CohRTA CohRTA Cohorte multicéntrica de personas adultas con trastorno por uso de alcohol que solicitan tratamiento por primera vez Estudio
III Jornada Alcohol y Alcoholismo SEMI Madrid, 26 Abril 2014 Estudio CohRTA CohRTA Cohorte multicéntrica de personas adultas con trastorno por uso de alcohol que solicitan tratamiento por primera vez Estudio
García Rueda A, Rodríguez Gil A, Bulo Concellón, R. UGC Servicio de Farmacia. Hospital Universitario Puerta del Mar, Cádiz
 ANÁLISIS DE UN PROGRAMA DE ATENCIÓN FARMACÉUTICA E IMPACTO EN LA SATISFACCIÓN DE LOS PACIENTES CON HEPATITIS C Vázquez Vela V, Huertas Fernández MJ, Domínguez Cantero M, Vázquez Vela V, Huertas Fernández
ANÁLISIS DE UN PROGRAMA DE ATENCIÓN FARMACÉUTICA E IMPACTO EN LA SATISFACCIÓN DE LOS PACIENTES CON HEPATITIS C Vázquez Vela V, Huertas Fernández MJ, Domínguez Cantero M, Vázquez Vela V, Huertas Fernández
Hepatitis C crónica en pacientes con infección por el VIH
 Actualización Hepatitis C crónica en pacientes con infección por el VIH Epidemiología pág.1 Historia natural pág.5 Trasplante hepático pág. 15 Puntos clave Todo paciente coinfectado debería ser considerado
Actualización Hepatitis C crónica en pacientes con infección por el VIH Epidemiología pág.1 Historia natural pág.5 Trasplante hepático pág. 15 Puntos clave Todo paciente coinfectado debería ser considerado
ACADEMIA DE FARMACIA DE CASTILLA Y LEÓN
 Resumen de la conferencia pronunciada por la Dra. Dª. Cristina Arenas Departamento Médico. Laboratorios Gilead con el título Situación actual del tratamiento farmacológico " Salamanca, 1 de Junio de 2015
Resumen de la conferencia pronunciada por la Dra. Dª. Cristina Arenas Departamento Médico. Laboratorios Gilead con el título Situación actual del tratamiento farmacológico " Salamanca, 1 de Junio de 2015
Características diferenciales de la población inmigrante con infección por VIH seguida en la consulta externa de un hospital universitario.
 Características diferenciales de la población inmigrante con infección por VIH seguida en la consulta externa de un hospital universitario. Characteristics of HIV-immigrant population under monitoring
Características diferenciales de la población inmigrante con infección por VIH seguida en la consulta externa de un hospital universitario. Characteristics of HIV-immigrant population under monitoring
Hepatitis aguda C en pacientes VIH. Montserrat Laguno Centeno Hospital Clínico. Barcelona 08/10/2015
 Hepatitis aguda C en pacientes VIH Montserrat Laguno Centeno Hospital Clínico. Barcelona 08/10/2015 Situación actual de la Hepatitis Aguda C (HAC) en el paciente VIH Experiencia en HAC en el paciente VIH
Hepatitis aguda C en pacientes VIH Montserrat Laguno Centeno Hospital Clínico. Barcelona 08/10/2015 Situación actual de la Hepatitis Aguda C (HAC) en el paciente VIH Experiencia en HAC en el paciente VIH
Profilaxis pre-exposición ( PrEP ): Estado actual e implicaciones
: Estado actual e implicaciones") Profilaxis pre-exposición ( PrEP ): Estado actual e implicaciones Alvaro Carrascal, MD, MPH Director, División de Atención de Salud Instituto del SIDA, Departamento de Salud del Estado de Nueva York Profesor
Profilaxis pre-exposición ( PrEP ): Estado actual e implicaciones Alvaro Carrascal, MD, MPH Director, División de Atención de Salud Instituto del SIDA, Departamento de Salud del Estado de Nueva York Profesor
Estudios sobre cuándo iniciar. Alberto La Rosa
 Estudios sobre cuándo iniciar TARGA Alberto La Rosa Cuándo comenzar TARGA? Mas de dos décadas de antiretrovriales pero aun no tenemos una respuesta definitiva a esta pregunta Visión clásica sobre relación
Estudios sobre cuándo iniciar TARGA Alberto La Rosa Cuándo comenzar TARGA? Mas de dos décadas de antiretrovriales pero aun no tenemos una respuesta definitiva a esta pregunta Visión clásica sobre relación
Aproximación terapéutica a la hepatitis por virus C
 COLUMNA DE HÍGADO Aproximación terapéutica a la hepatitis por virus C Therapeutic approach to hepatitis for virus C Víctor Idrovo C. MD. 1 RESUMEN La hepatitis C (VHC) es producida por un virus RNA perteneciente
COLUMNA DE HÍGADO Aproximación terapéutica a la hepatitis por virus C Therapeutic approach to hepatitis for virus C Víctor Idrovo C. MD. 1 RESUMEN La hepatitis C (VHC) es producida por un virus RNA perteneciente
PROTOCOLO DE PROFILAXIS POST-EXPOSICIÓN FRENTE A VIH
 PROTOCOLO DE PROFILAXIS POST-EXPOSICIÓN FRENTE A VIH Ante paciente que acude por posible contacto con VIH, o personal sanitario en contacto potencial con el virus, se recomienda seguir el siguiente algoritmo
PROTOCOLO DE PROFILAXIS POST-EXPOSICIÓN FRENTE A VIH Ante paciente que acude por posible contacto con VIH, o personal sanitario en contacto potencial con el virus, se recomienda seguir el siguiente algoritmo
Enfermedad Cardiovascular en Trasplante Renal. Dr. Alberto Flores Almonte. Nefrólogo. Unidad de Uro-Nefrología y Trasplante renal. CEDIMAT.
 Enfermedad Cardiovascular en Trasplante Renal. Dr. Alberto Flores Almonte. Nefrólogo. Unidad de Uro-Nefrología y Trasplante renal. CEDIMAT. Enfermedad Cardiovascular. Causa principal de morbimortalidad
Enfermedad Cardiovascular en Trasplante Renal. Dr. Alberto Flores Almonte. Nefrólogo. Unidad de Uro-Nefrología y Trasplante renal. CEDIMAT. Enfermedad Cardiovascular. Causa principal de morbimortalidad
BIBLIOGRAFÍA COMENTADA
 BIBLIOGRAFÍA COMENTADA Gastroenterology An IL-28B polymorphism determines treatment response of hepatitis C virus genotype 2 or 3 patients who do not achieve a rapid virologic response Un polimorfismo
BIBLIOGRAFÍA COMENTADA Gastroenterology An IL-28B polymorphism determines treatment response of hepatitis C virus genotype 2 or 3 patients who do not achieve a rapid virologic response Un polimorfismo
Tratamiento de la hepatitis C recurrente post-trasplante. Cuando y Como. Victoria Aguilera XXVI Congreso SETH 2-4 Octubre de 2013 Córdoba
 Tratamiento de la hepatitis C recurrente post-trasplante. Cuando y Como Victoria Aguilera XXVI Congreso SETH 2-4 Octubre de 2013 Córdoba Indicación de TH por cirrosis VHC y Supervivencia post-th Historia
Tratamiento de la hepatitis C recurrente post-trasplante. Cuando y Como Victoria Aguilera XXVI Congreso SETH 2-4 Octubre de 2013 Córdoba Indicación de TH por cirrosis VHC y Supervivencia post-th Historia
Tratamiento de la hepatitis crónica C genotipo 2 y 3 en 2015
 Tratamiento de la hepatitis crónica C genotipo 2 y 3 en 2015 Ricard Solà Hospital del Mar Barcelona 22 de Mayo de 2015 Med Clin (Barc) 2002; 119: 90-95. Prevalencia de los distintos genotipos del virus
Tratamiento de la hepatitis crónica C genotipo 2 y 3 en 2015 Ricard Solà Hospital del Mar Barcelona 22 de Mayo de 2015 Med Clin (Barc) 2002; 119: 90-95. Prevalencia de los distintos genotipos del virus
VHB Y VHC EN EL EMBARAZO. Senador Morán Sánchez Servicio de Digestivo HUSL
 VHB Y VHC EN EL EMBARAZO Senador Morán Sánchez Servicio de Digestivo HUSL IMPORTANCIA DE LA INFECCION CONSECUENCIAS CLINICAS VHC MORBILIDAD Y MORTALIDAD VHC HIV Accidente trafico 12 muertes al dia 3 muertes
VHB Y VHC EN EL EMBARAZO Senador Morán Sánchez Servicio de Digestivo HUSL IMPORTANCIA DE LA INFECCION CONSECUENCIAS CLINICAS VHC MORBILIDAD Y MORTALIDAD VHC HIV Accidente trafico 12 muertes al dia 3 muertes
Vacunación antihepatitis B en el paciente con VIH
 José Ángel Rodrigo Pendás Servicio de Medicina Preventiva y Epidemiología Hospital Vall d Hebron 24 de abril de 2008 Contenido Importancia de la vacunación antihepatitis B en personas con VIH Inmunogenicidad
José Ángel Rodrigo Pendás Servicio de Medicina Preventiva y Epidemiología Hospital Vall d Hebron 24 de abril de 2008 Contenido Importancia de la vacunación antihepatitis B en personas con VIH Inmunogenicidad
SIMEPREVIR Infección por el virus de la hepatitis C
 GENESIS-SEFH Versión: 4.0 Programa MADRE versión 4.0 Fecha: 10-12-2012 Informe Base Página: 1 SIMEPREVIR Infección por el virus de la hepatitis C (Informe para la CURMP) Fecha: Septiembre 2014 Glosario:
GENESIS-SEFH Versión: 4.0 Programa MADRE versión 4.0 Fecha: 10-12-2012 Informe Base Página: 1 SIMEPREVIR Infección por el virus de la hepatitis C (Informe para la CURMP) Fecha: Septiembre 2014 Glosario:
Coinfección VIH y Hepatitis C Trasplante hepático. María de los Remedios Alemán Valls Hospital Universitario de Canarias
 Coinfección VIH y Hepatitis C Trasplante hepático María de los Remedios Alemán Valls Hospital Universitario de Canarias HIV y enfermedad hepática Enfermedades oportunistas Cacaína, heroína Virus de hepatitis
Coinfección VIH y Hepatitis C Trasplante hepático María de los Remedios Alemán Valls Hospital Universitario de Canarias HIV y enfermedad hepática Enfermedades oportunistas Cacaína, heroína Virus de hepatitis
RESUMEN EJECUTIVO EN ESPAÑOL
 RESUMEN EJECUTIVO EN ESPAÑOL Guía de Práctica Clínica para la prevención, diagnóstico, evaluación y tratamiento de la Hepatitis C en enfermedad renal crónica Page 1 of 8 GUIA 1: DETECCIÓN Y EVALUACIÓN
RESUMEN EJECUTIVO EN ESPAÑOL Guía de Práctica Clínica para la prevención, diagnóstico, evaluación y tratamiento de la Hepatitis C en enfermedad renal crónica Page 1 of 8 GUIA 1: DETECCIÓN Y EVALUACIÓN
Originales. Efectividad y seguridad de los antivirales de acción directa frente al virus de la hepatitis C. Revista de la OFIL
 Originales Efectividad y seguridad de los antivirales de acción directa frente al virus de la hepatitis C Revista de la OFIL Rev. OFIL 2016, 26;4:243-250 Fecha de recepción: 12/08/2016 - Fecha de aceptación:
Originales Efectividad y seguridad de los antivirales de acción directa frente al virus de la hepatitis C Revista de la OFIL Rev. OFIL 2016, 26;4:243-250 Fecha de recepción: 12/08/2016 - Fecha de aceptación:
Debemos Tratar la Hepatitis Crónica B en el Paciente Inmunotolerantey en el Portador Inactivo?
 Debemos Tratar la Hepatitis Crónica B en el Paciente Inmunotolerantey en el Portador Inactivo? X Curso Avances en Infección por VIH y Hepatitis Virales A Coruña, 6 de Febrero de 2016 Berta Pernas Souto
Debemos Tratar la Hepatitis Crónica B en el Paciente Inmunotolerantey en el Portador Inactivo? X Curso Avances en Infección por VIH y Hepatitis Virales A Coruña, 6 de Febrero de 2016 Berta Pernas Souto
XXI Congreso de la Sociedad Española de Trasplante Hepático (SETH). Badajoz, 7-9 de Octubre de 2.009
. Badajoz, 7-9 de Octubre de 2.009") XXI Congreso de la Sociedad Española de Trasplante Hepático (SETH). Badajoz, 7-9 de Octubre de 2.009 LA PROLONGACIÓN DEL TRATAMIENTO ANTIVIRAL EN LA HEPATITIS POR VIRUS C RECURRENTE POSTRASPLANTE HEPÁTICO
XXI Congreso de la Sociedad Española de Trasplante Hepático (SETH). Badajoz, 7-9 de Octubre de 2.009 LA PROLONGACIÓN DEL TRATAMIENTO ANTIVIRAL EN LA HEPATITIS POR VIRUS C RECURRENTE POSTRASPLANTE HEPÁTICO
Edward Cachay MD, MAS Associate Professor of Medicine UCSD Owen Clinic La Coruña Febrero 2013
 Edward Cachay MD, MAS Associate Professor of Medicine UCSD Owen Clinic La Coruña Febrero 2013 Agenda Importancia y caracterización de las reacciones adversas asociadas al tratamiento de la hepatitis C
Edward Cachay MD, MAS Associate Professor of Medicine UCSD Owen Clinic La Coruña Febrero 2013 Agenda Importancia y caracterización de las reacciones adversas asociadas al tratamiento de la hepatitis C
Meningitis Tuberculosa y su Tratamiento Santiago Moreno Hospital Ramón y Cajal. IRYCIS. Madrid
 Taller UITB 2012 Barcelona, 19-20 de Noviembre de 2012 Meningitis Tuberculosa y su Tratamiento Santiago Moreno Hospital Ramón y Cajal. IRYCIS. Madrid Meningitis tuberculosa Importancia Presentación clínica
Taller UITB 2012 Barcelona, 19-20 de Noviembre de 2012 Meningitis Tuberculosa y su Tratamiento Santiago Moreno Hospital Ramón y Cajal. IRYCIS. Madrid Meningitis tuberculosa Importancia Presentación clínica
Informe de Posicionamiento Terapéutico de Sofosbuvir (Sovaldi )
") INFORME DE POSICIONAMIENTO TERAPÉUTICO PT-SOFOSBUVIR/V1/01112014 Informe de Posicionamiento Terapéutico de Sofosbuvir (Sovaldi ) Fecha de publicación: 18 de Noviembre de 2014 La infección por el virus
INFORME DE POSICIONAMIENTO TERAPÉUTICO PT-SOFOSBUVIR/V1/01112014 Informe de Posicionamiento Terapéutico de Sofosbuvir (Sovaldi ) Fecha de publicación: 18 de Noviembre de 2014 La infección por el virus
Nadia Isabel Hornquist Hurtarte Química Bióloga Clínica de Enfermedades Infecciosas Hospital Roosevelt
 Nadia Isabel Hornquist Hurtarte Química Bióloga Clínica de Enfermedades Infecciosas Hospital Roosevelt Fase aguda: Entre el 40% a 90% sintomáticos (similar mononucleosis) Fase crónica: asintomaticos El
Nadia Isabel Hornquist Hurtarte Química Bióloga Clínica de Enfermedades Infecciosas Hospital Roosevelt Fase aguda: Entre el 40% a 90% sintomáticos (similar mononucleosis) Fase crónica: asintomaticos El
ACTUALIZACIÓN DE JUNIO 2015. PANELES DE EXPERTOS DE LOS GRUPOS GEHEP Y GeSIDA
 ACTUALIZACIÓN DE JUNIO 2015 PANELES DE EXPERTOS DE LOS GRUPOS GEHEP Y GeSIDA RECOMENDACIONES DE TRATAMIENTO EN PACIENTES CON GENOTIPO 1 PACIENTES SIN TRATAMIENTO PREVIO Sofosbuvir/Ledipasvir a. Recomendación
ACTUALIZACIÓN DE JUNIO 2015 PANELES DE EXPERTOS DE LOS GRUPOS GEHEP Y GeSIDA RECOMENDACIONES DE TRATAMIENTO EN PACIENTES CON GENOTIPO 1 PACIENTES SIN TRATAMIENTO PREVIO Sofosbuvir/Ledipasvir a. Recomendación
Familia: Retroviridae. Género: Lentivirus. Diámetro: 120 nm. Especies: HIV 1, HIV 2. Genoma: 2 ARN monocatenarios positivos.
 30 de Agosto 2010 Bioq. Alvarez, Juliana Bioq. Archuby, Daniela El Síndrome S Inflamatorio de Reconstitución Inmunológica (IRIS), ocurre en una subpoblación n de pacientes infectados por HIV (10-30%) durante
30 de Agosto 2010 Bioq. Alvarez, Juliana Bioq. Archuby, Daniela El Síndrome S Inflamatorio de Reconstitución Inmunológica (IRIS), ocurre en una subpoblación n de pacientes infectados por HIV (10-30%) durante
BIBLIOGRAFÍA INTERNACIONAL
 BIBLIOGRAFÍA INTERNACIONAL Clinical infectious diseases Comparison of the early fungicidal activity of high-dose fluconazole, voriconazole, and flucytosine as secondline drugs given in combination with
BIBLIOGRAFÍA INTERNACIONAL Clinical infectious diseases Comparison of the early fungicidal activity of high-dose fluconazole, voriconazole, and flucytosine as secondline drugs given in combination with
Costo efectividad de la vacunación contra enfermedad neumocóccica en mayores de 60 años en Colombia Nelson Alvis Guzman PhD
 Costo efectividad de la vacunación contra enfermedad neumocóccica en mayores de 60 años en Colombia Nelson Alvis Guzman PhD Evaluación Económica de Vacunas Es el uso herramientas analíticas para generar
Costo efectividad de la vacunación contra enfermedad neumocóccica en mayores de 60 años en Colombia Nelson Alvis Guzman PhD Evaluación Económica de Vacunas Es el uso herramientas analíticas para generar
SEIMC2014. Infecciones micobacterianas en el paciente con trasplante de órgano sólido y progenitores hematopoyéticos
 Infecciones micobacterianas en el paciente con trasplante de órgano sólido y progenitores hematopoyéticos Dr. Julián de la Torre Cisneros. Unidad de Enfermedades Infecciosas Hospital Universitario Reina
Infecciones micobacterianas en el paciente con trasplante de órgano sólido y progenitores hematopoyéticos Dr. Julián de la Torre Cisneros. Unidad de Enfermedades Infecciosas Hospital Universitario Reina
VIH Y EMBARAZO TALLER NACIONAL DE LA ELIMINACIÓN MATENRO INFANTIL DEL VIH D R A. C L A U D I A M A Z A R I E G O S
 VIH Y EMBARAZO TALLER NACIONAL DE LA ELIMINACIÓN MATENRO INFANTIL DEL VIH D R A. C L A U D I A M A Z A R I E G O S Guatemala 2 de marzo de 2016 PERSONAS CON EL VIH CON ACCESO AL TRATAMIENTO RICO En junio
VIH Y EMBARAZO TALLER NACIONAL DE LA ELIMINACIÓN MATENRO INFANTIL DEL VIH D R A. C L A U D I A M A Z A R I E G O S Guatemala 2 de marzo de 2016 PERSONAS CON EL VIH CON ACCESO AL TRATAMIENTO RICO En junio
FishmanJA, RubinRH. N Engl J Med 1998;338:1741-51. Epidemiología. Experts, acollidors i solidaris
 INFECCIÓN TARDIA i T.O.S. Albert Pahissa Servicio Enfermedades Infecciosas. H. Vall d Hebron Universitat Autónoma de Barcelona FishmanJA, RubinRH. N Engl J Med 1998;338:1741-51. Epidemiología Timetable
INFECCIÓN TARDIA i T.O.S. Albert Pahissa Servicio Enfermedades Infecciosas. H. Vall d Hebron Universitat Autónoma de Barcelona FishmanJA, RubinRH. N Engl J Med 1998;338:1741-51. Epidemiología Timetable
Autoridades. Presidenta de la Nación Dra. Cristina Fernandez de Kirchner. Ministro de Salud Dr. Juan Luis Manzur
 Autoridades Presidenta de la Nación Dra. Cristina Fernandez de Kirchner Ministro de Salud Dr. Juan Luis Manzur Secretario de Promoción y Programas Sanitarios Dr. Máximo Andrés Diosque Subsecretaria de
Autoridades Presidenta de la Nación Dra. Cristina Fernandez de Kirchner Ministro de Salud Dr. Juan Luis Manzur Secretario de Promoción y Programas Sanitarios Dr. Máximo Andrés Diosque Subsecretaria de
Ficha descriptiva sobre gestión Por qué las pruebas de VIH gratuitas confidenciales y voluntarias tienen que ser una prioridad nacional.
 Ficha descriptiva sobre gestión Por qué las pruebas de VIH gratuitas confidenciales y voluntarias tienen que ser una prioridad nacional. Hechos El incremento del acceso y la aceptación de las pruebas precoces
Ficha descriptiva sobre gestión Por qué las pruebas de VIH gratuitas confidenciales y voluntarias tienen que ser una prioridad nacional. Hechos El incremento del acceso y la aceptación de las pruebas precoces
OLYSIO SIMEPREVIR 150 mg Cápsulas. Grupo farmacoterapéutico: antivirales para uso sistémico, antivirales de acción directa, código ATC: J05AE14
 OLYSIO SIMEPREVIR 150 mg Cápsulas Industria Italiana Administración por vía oral Venta bajo receta archivada FORMULA CUALI Y CUANTITATIVA Cada cápsula de Olysio contiene: Simeprevir 150 mg (correspondiente
OLYSIO SIMEPREVIR 150 mg Cápsulas Industria Italiana Administración por vía oral Venta bajo receta archivada FORMULA CUALI Y CUANTITATIVA Cada cápsula de Olysio contiene: Simeprevir 150 mg (correspondiente
Tratamiento de la hepatitis crónica por virus C en grupos especiales
 Tratamiento de la hepatitis crónica por virus C en grupos especiales Carlos Fernández Carrillo, José Luis Calleja Panero Hospital Universitario Puerta de Hierro, Majadahonda. Universidad Autónoma de Madrid
Tratamiento de la hepatitis crónica por virus C en grupos especiales Carlos Fernández Carrillo, José Luis Calleja Panero Hospital Universitario Puerta de Hierro, Majadahonda. Universidad Autónoma de Madrid
AVANCES EN LA INFECCIÓN VIH EN PEDIATRIA
 AVANCES EN LA INFECCIÓN VIH EN PEDIATRIA Juncal Echeverria Lecuona Neonatologia. Hospital Donostia En la tercera decada de la infección VIH, las nuevas terapias antirretrovirales han transformado la enfermedad
AVANCES EN LA INFECCIÓN VIH EN PEDIATRIA Juncal Echeverria Lecuona Neonatologia. Hospital Donostia En la tercera decada de la infección VIH, las nuevas terapias antirretrovirales han transformado la enfermedad
Efectividad de la triple terapia con telaprevir en la hepatitis C crónica en pacientes monoinfectados y coinfectados
 Vol. 24 Nº 2 2014 Efectividad de la triple terapia con telaprevir en la hepatitis C crónica en pacientes monoinfectados y coinfectados Rev. O.F.I.L. 2014, 24;2:80-85 SANGRADOR PELLUZ C 1, SOLER COMPANY
Vol. 24 Nº 2 2014 Efectividad de la triple terapia con telaprevir en la hepatitis C crónica en pacientes monoinfectados y coinfectados Rev. O.F.I.L. 2014, 24;2:80-85 SANGRADOR PELLUZ C 1, SOLER COMPANY
Juan E. Losa. Hospital U. F. Alcorcón. Universidad Rey Juan Carlos. Es posible diagnosticar antes el VIH en Medicina Interna?
 Juan E. Losa. Hospital U. F. Alcorcón. Universidad Rey Juan Carlos. Es posible diagnosticar antes el VIH en Medicina Interna? Guión 1. Presentación tardía 2. Necesidad de diagnóstico precoz 3. Suficiente
Juan E. Losa. Hospital U. F. Alcorcón. Universidad Rey Juan Carlos. Es posible diagnosticar antes el VIH en Medicina Interna? Guión 1. Presentación tardía 2. Necesidad de diagnóstico precoz 3. Suficiente
Epidemiología de la hepatitis B y hepatitis C en el trasplante renal
 Virus hepatotropos - Ponencia Epidemiología de la hepatitis B y hepatitis C en el trasplante renal José María Morales Servicio de Nefrología. Unidad de Trasplante Renal Hospital 12 de Octubre, Madrid INTRODUCCIÓN
Virus hepatotropos - Ponencia Epidemiología de la hepatitis B y hepatitis C en el trasplante renal José María Morales Servicio de Nefrología. Unidad de Trasplante Renal Hospital 12 de Octubre, Madrid INTRODUCCIÓN