Expresión de PD-L1 como Factor Predictivo de Respuesta: Resultados Clínicos con Inmunoterapia Dolores Isla Servicio de Oncología Médica HCU Lozano
|
|
|
- María Cristina de la Fuente Mora
- hace 7 años
- Vistas:
Transcripción
1 Expresión de PD-L1 como Factor Predictivo de Respuesta: Resultados Clínicos con Inmunoterapia Dolores Isla Servicio de Oncología Médica HCU Lozano Blesa de Zaragoza

2

3
4 Immune Checkpoint Inhibitors
5 Biomarkers and Immunotherapy Immunotherapy Targeted Therapy Efficacy of Immunotherapy defined by long lasting tumor stabilization Purpose of Biomarker development in Immunotherapy: A Biomarker to identify patients with high benefit A Biomarker to exclude patients without benefit Currently both strategies are under exploration
6 Introduction New era of Precision Medicine, searching a predictive biomarker to select real p. who would benefit from checkpoint blockades is crucial: to prevent them from autoimmune adverse effects high cost
7 Predictive Role of PD-L1 expression PD-L1 is up-regulated in selected solid tumors and it can be detected by IHC on TCs and ICs The association of PD-L1 expression and the efficacy of PD-1/PD-L1 checkpoint blockades are investigated in a lot of studies
8
9 Association of PD-L1 expression with immune response of anti PD-1/PD-L1 Ab

10
11 Lancet 2015 HR=0.71, p= (2 mg/kg) HR=0.61, p= (10 mg/kg) PD-L1 as a Predictive Marker
12 CASO CLÍNICO Varón, 61 años HTA, Dislipemia desde 2012 Exfumador desde hace 2 años, IPA=15 Abril/2013: nódulos subcutáneos a nivel lumbar y torácico dcho de 2 m. de evolución EXPLORACIÓN FÍSICA: Múltiples letálides y nódulos en región torácica dcha, axilar dcha, subpectoral dcho, pared abdominal, lumbar ANALÍTICA: LDH 753 U/L MARCADORES TUMORALES: Enolasa 24 ng/ml TAC cérvico-torácico-abdomino-pélvico: Nódulo LSI 2,5 cms Lesión subpectoral dcha 5 cms Adenopatía axilar dcha 2,5 cms Lesión subescapular dcha 5 cms Nódulo suprarrenal dcho 1,2 cms Nódulo suprarrenal izdo 3,8 cms Lesión hepática 3 cms Lesión m. recto anterior 2,5 cms Lesión lumbar 3 cms TAC cerebral: Normal GAMMAGRAFÍA ÓSEA: metástasis óseas en D8 y tibia dcha
13 PRUEBAS COMPLEMENTARIAS PET-TC: Nódulo LSI SUVmax 5,6 Nódulo suprarrenal dcho SUVmax 8,1 Nódulo suprarrenal izdo SUVmax 6 Lesión hepática SUVmax 6,8 Metástasis en D8 SUVmax 7 Adenopatías supraclaviculares, axilar dcha, abdominales, iliacas, inguinales con SUVmax hasta 13,2 Masas a nivel muscular subescapular dcha, recto anterior dcho, paravertebrales, glúteos Masas subcutáneas pared torácica, pared abdominal, lumbar, EEII SUVmax hasta 11,6
14 PET-TC Mayo/2013
15 PRUEBAS COMPLEMENTARIAS PAAF nódulo subcutáneo subescapular dcho: carcinoma poco diferenciado BIOPSIA masa m. recto anterior: Carcinoma Indiferenciado de alto grado de posible origen pulmonar (No Microcítico, posible Adenocarcinoma): IHQ: Ki 67 90% CK7 + TTF1 P63 Enolasa, Sinaptofisina, Cromogranina Resto (melanoma, linfoma, ): Mutación EGFR: Translocación ALK: Fractura patológica tibia dcha: Junio 2013

16 1ª LÍNEA DE TRATAMIENTO CARBOPLATINO AUC:6 iv día 1 PACLITAXEL 200 mg/m 2 iv día 1 BEVACIZUMAB 15 mg/kg iv día 1 (1 ciclo) Cada 21 días x 6 ciclos PEMETREXED 500 mg/m 2 iv día 1 x 1 ciclo + Ac. Zoledrónico 4 mg iv/21 días Mayo/2013 a Noviembre/2013 RESPUESTA PARCIAL

17 2ª LÍNEA DE TRATAMIENTO GEMCITABINA 1500 mg/m 2 iv día 1 Cada 15 días x 10 ciclos + Ac. Zoledrónico 4 mg iv/28 días Diciembre/2013 a Abril/2014 ENFERMEDAD ESTABLE
18 TAC Mayo/2014 TAC cérvico-torácico-abdomino-pélvico: Nódulo LSI 1,6 x 2 cms Adenopatía supraclavicular dcha 4,5 x 4,5 cms Adenopatía axilar dcha 6 x 6 cms Lesión subescapular dcha 9 x 5 cms Nódulo suprarrenal dcho 1,2 x 0,8 cms Nódulo suprarrenal izdo 3,2 x 1,5 cms Lesión m. recto anterior 2 x 2 cms Lesión m. oblícuo externo 1,5 x 1 cms Lesión m. glúteo mayor izdo 3,5 x 3 cms Nódulo pancreático 1 x 1 cm
19 TAC Mayo/2014
20 TAC Mayo/2014
21 3ª LÍNEA DE TRATAMIENTO KEYNOTE 010 Randomized Study of Pembrolizumab vs. Docetaxel in Patients with Previously Treated PD L1 Positive* NSCLC Patients: (n = 920) Metastatic NSCLC Previously treated (progression after 2 cycles of platinum doublet OR prior EGFR TKI in mutant) Measurable disease ECOG PS 0 1 Newly obtained formalin fixed specimens strongly encouraged PD L1 Positive (defined as staining in 1% of tumor cells) No CNS metastases hgu R A N D O M I Z A T I O N 1:1:1 N=920 R 1:1:1 Pembrolizumab 2 mg/kg Q3W Pembrolizumab 10 mg/kg Q3W Docetaxel 75 mg/m2 Q3W Primary Endpoints: OS, PFS, Safety (adverse events and drug discontinuation) Secondary Endpoints: ORR and response duration (RECIST 1.1) a Positive defined as 1% tumor PD-L1 expression determined using a prototype IHC assay (22C3 antibody). 52 Mayo/2014 a HOY
22 TAC Julio/2014
23 TAC Julio/2014
24 TAC Enero/2015
25 TAC Marzo/2016
26 EVOLUCIÓN CICLOS: 33 (max. 35 sin PR y suspender tto hasta PR por IrRC) CLÍNICA: desaparición completa de letálides/nódulos. Asintomático TOXICIDAD: Ninguna RESPUESTA (irrc): RP: Basal: mm 2 C4: mm 2 : RP ( 50% disminución tumor respecto de superficie basal) C7: 360 mm 2 C10: 450 mm 2 C13: 311 mm 2 C23: 229 mm2,... SLP: 23 meses (3,9 m en Estudio KEYNOTE 010) SG: 35 meses (10,4 m en Estudio KEYNOTE 010)


27
28 SE DEBE CONSIDERAR LA EXPRESIÓN DE PD-L1 SÓLO EN ADENOCARCINOMA DE PULMÓN? 1. SI 2. NO 3. SÓLO CON PEMBROLIZUMAB 4. SÓLO CON NIVOLUMAB
 HR=0.61, p=0.")
29 Lancet 2015 HR=0.71, p= (2 mg/kg) HR=0.61, p= (10 mg/kg)

30 NSCLC

31 N= 3790 p.? YES 1. Benefit from PD-1 inhibitors versus docetaxel in second line treatment of NSCLC is limited to the PD-L1 > 1% subpopulation. 2. Potential benefit from PD-1/PD-L1 targeted agents does exist with higher intensity associated with higher ORR. NO JAMA Oncology 2016

32 N=1979 p. 24-weeks PFS Aguiar P, 2016

33 N=914 p.

34
35
36 Association of PD-L1 expression with immune response of anti PD-1/PD-L1 Ab Wide variability of PD-L1 expression is observed in different tumor types The overexpression of PD-L1 is significantly associated with better response to PD-1/PD-L1 blockade in: Melanoma NSCLC: Pembrolizumab, Nivolumab (non-squamous), Atezolizumab Bladder cancer Ovarian cancer Others
37 Association of PD-L1 expression with immune response of anti PD-1/PD-L1 Ab Some studies have shown the efficacy of PD- 1/PD-L1 antibodies independent of PD-L1 expression: Advanced RCC and Nivolumab Squamous NSCLC and Nivolumab
38 N= 1475 p. 20 trials (not very updated) ORR= 34,1% vs 19,9%, p< PLoS One 2015
39 Carbognin L, PLoS One 2015

40 N=5959 p. (MM, NSCLC, RCC)

41 Sunshine J, Curr Opin Pharmacol 2015

42 Lancet 2015

43

44 We observed cogain or coamplification of CD274 and PDCD1LG2 in 32 of 48 cervical SCCs (67%) and 10 of 23 vulvar SCCs (43%). Median PD-L1 protein expression was highest among tumors with CD274 and PDCD1LG2 coamplification and lowest among tumors with disomy. J Thorac Oncol 2015
45 Prognostic Role of PD-L1 expression on Lung Cancer Cells

46

47 PD-L1 expression on TCs and ICs Multiple studies with PD-L1 expression on TCs and ICs as a predictor of response to PD-1/PD-L1 checkpoint blockades
48 PD-L1 expression on TCs and ICs Not all tumors show simultaneous PD-L1 positive both on TCs and ICs Which is more important in predicting the response? TCs was correlated significantly with ORR and clinical benefit to anti-pd-1 therapy ICs with ORR that does not reach the statistical significance in multiple solid cancers, but not always (genitourinary cancer)
49 Herbst R, Nature 2014
50 Dynamic PD-L1 expression Expression of PD-L1 can be induced by activated tumor antigenspecific T cells: dynamic process during the recognition of effective T-cell antigen (Taube et al, Sci Transl Med 2012) Microsatellite instability high (MSI-H) colorectal cancer can attract TILs and upregulate PD-L1 expression in tumor (Gatalica et al, Cancer Epidemiol Biomarkers Prev 2014) Potential inducibility of PD-L1 expression by First-line CT Increased PD-L1 expression in the serial tumor biopsy during the Atezolizumab therapy exhibited accompanied with ORR TKI-targeted therapy: compared in pre- and post-tki biopsies in EGFR-mutant and ALKpositive metastatic NSCLC expression levels of PD-L1 in biopsies changed due to TKI therapy (22% and 25%) (Gainor et al, J Clin Oncol 2015) Evaluation at a single time point may not reflect an evolving immune response or predict response to PD-1/PD-L1 inh.


51 PD-L1 expression is Dynamic and may change after exposure to Treatment Baseline On-treatment CD8 T-cells PD-L1 CD8 T-cells PD-L1 MPDL3280A (PD-L1 inhibitor) T-cells and tumor cells expressing PD- L1 PD-L1 = programmed cell death-ligand 1. Powderly J, et al. Oral presentation at ASCO 2013 (abstr. 3001).
52 Prior TKI Therapy in NSCLC EGFR Mutant Patients Associates with Lack of Response to Anti-PD-1 Treatment Study objective To determine the relationship between prior TKI therapy and response to anti-pd-1 therapy in patients with NSCLC EGFR mutations (EGFRm) Study design In vitro Western blot analysis of PD-L1 expression in NSCLC cell lines in response to erlotinib and afatinib Clinical Retrospective analysis of patients from KEYNOTE-001 clinical trial in which patients received pembrolizumab 2 mg/kg q3w or 10 mg/kg q2 3w IMMUNOTHERAPY and Key results In vitro PD-L1 levels decrease in response to EGFR TKI in cell lines sensitive to TKI Clinical EGFR mut + p.: Among 29 EGFRm patients in KEYNOTE-001, 2 of 3 EGFR-naïve patients achieved a PR vs. 1 of 26 with a history of prior EGFR Wait TKI (p<0.001) and See situation 18 of these patients had a 9-week follow-up scan Both of the EGFR TKI-naïve patients achieved a PR compared with only 1 of 16 with a history of prior EGFR TKI (p<0.001) In EGFR wild-type patients, prior TKI did not affect RR (p<0.601) A lower proportion (perhaps of EGFRm patients continued for on trial to PD-L1 the 9-week scan (62% +) [18/29]), compared with EGFR wild-type patients (87% [60/69]) Conclusions There was a strong correlation between response and lack of prior EGFR TKI treatment, especially in those with a sensitising mutation PD-L1 levels decreased in response to an EGFR in cell lines sensitive to TKI PD-1/PD-L1 inhibition prior to an EGFR TKI may be more efficacious than a strategy in which the PD-1/PD-L1 inhibition follows, or is given concurrently with an EGFR TKI Garon et al. J Thorac Oncol 2015
53 SE DEBE REBIOPSIAR PARA CONOCER LA EXPRESIÓN DE PD-L1? 1. SI 2. NO 3. SÓLO CON PEMBROLIZUMAB 4. SÓLO CON NIVOLUMAB

54 Rebiopsy?? Lancet S PFS NOT NOT
55 Heterogeneity of PD-L1 expression intra-patient Frequently discordant between primary tumor and metastasis (melanoma, RCC, NSCLC) Different expression levels in different lesions intra-patient (melanoma)
56
57 CORE 4 CORE 3 CORE 2 AQUA scores CORE 1 Intra-tumour and intra-patient heterogeneity PD-L1 expression can vary between different sites within the primary tumour There is only a weak correlation between PD-L1 expression in the primary tumour and the metastases Cytokeratin DAPI PD-L1 P = Cytokeratin DAPI PD-L Cytokeratin DAPI PD-L Cytokeratin DAPI PD-L1 Metastatic Primary PD-L1 expression (red) in 4 sites within the same primary RCC tumour PD-L1 expression in metastatic and primary specimens from patients with mrcc Jilaveanu LB, et al. J Cancer. 2014;5(3):
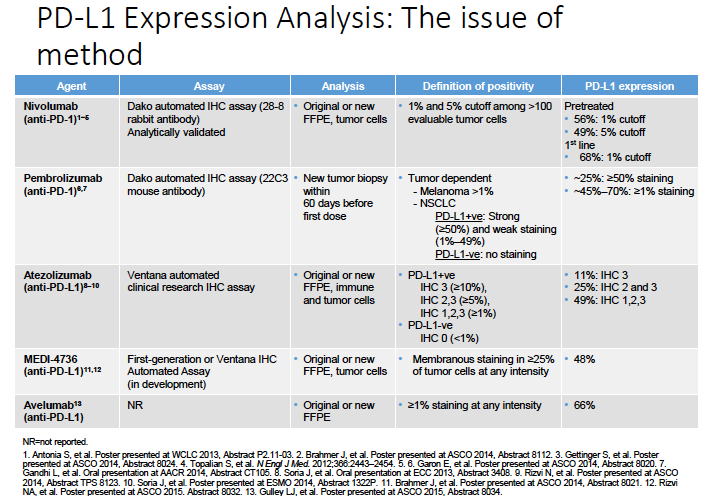
58 Reliability of detection methods PD-L1 expression in human cancers is usually investigated using the anti-pd-l1 antibody by IHC staining in formalin-fixed paraffin-embedded tissue samples Different anti-pd-l1 mabs and staining techniques (manual vs automated techniques) may result in different positive rates for TCs or ICs Limitations for IHC assay, but it is cheap and easy to conduct FISH??

59
60 DAKO
61 What is the reasonable Cut-off value? Cut-off values of 1%, 5%, 10%, 25% or 50% are frequently used to define the positive rate of PD-L1 staining Different cut-off values may lead to the difference in predicting function No clear definition for PD-L1 positive rate limits the validation of PD-L1 as a predictor to PD-1/PD-L1 checkpoint blockades It may not be reasonable to make consistent cut-off value for all tumors However, it is difficult to decide the cut-off value according to different cancers because there are: so many kinds of cancers various biological properties in the same cancer, especially for NSCLC
62 Target prevalence in Solid Tumors Solid Tumors??? PD-L
63 Efforts to identify determinants of Response with Immunotherapy PD-L1 Expression (TCs or ICs) CD8+ Tumor Infiltrating Lymphocytes (TILs) BCL-2-interacting mediator of cell death-bim (melanoma) Interferon-γ (melanoma, Durvalumab) PD-L2 expression (Pembrolizumab) Mutation / Neoantigen Burden / Mismatch-repair status / Microsatellite Instability / JAK2-3 genes Immune gene messenger RNA expression signatures Smoking Status
64 Immunotherapy and EGFR or RAS mut + Checkmate 057 Study Borghaei N, NEJM 2015
65

66 Immunotherapy and EGFR mut + KEYNOTE-010 Study Herbst R, Lancet 2015

67 Median 6,4 m. Mutation burden correlates with immune response and is higher with mismatch-repair deficiency Median NR Le DT, NEJM 2015
68 Are we ready to Select Patients?

69 Translational view of the complex patient-tumor immune interactions
70 PD-L1 as a Good Predictive Marker? PD-L1 expression is enriching for p. who respond to single agent PD-1 inh., but there are high levels of false negative (response with negative test) Assay dependent: Propietary antibody used Laboratory performing the assay Scoring methodology Tumor dependent: Sampling: Surgical vs biopsy Archival vs fresh Heterogeneity Tumor biology
71 PD-L1 expression by IHC Positive Predictive Value Negative Predictive Value
72 Challenges with PD-L1 Assessment TCs and/or ICs PD-L1 expression may change over time Fresh tumor or archival samples: rebiopsy? Tumor heterogeneity Reliability of detection methods Different IHC mab for PD-L1 positivity: multiple clones What cut-off (1 vs 5 vs 10 vs 50%)? Care when using in combination with other therapies, which may impact the predictive value of PD-L1 Randomized trials with PD-L1 stratification awaited
73 Clinical Trial Design in Checkpoint Blockades Identification of Predictive Biomarkers: Precision Medicine Pembrolizumab and NSCLC: Other possible biomarkers much be explored in clinical trials

74
75
76 One standardized assay

77
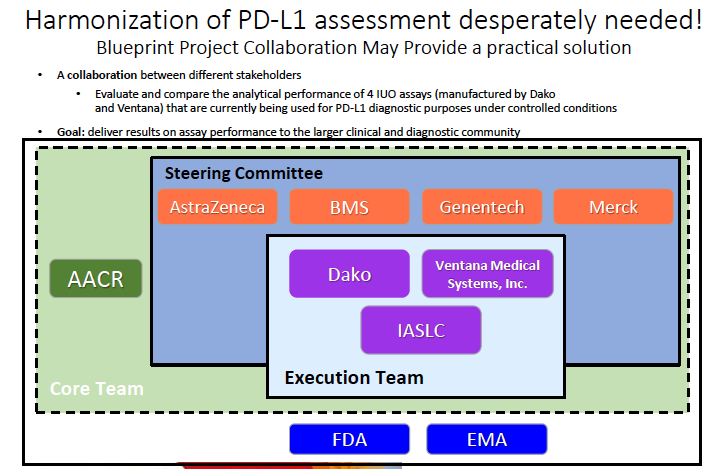
78 Conclusions IHC-based PD-L1 expression on TCs and/or ICs is an important but not a definitive predictive biomarker for the response to PD-1/PD-L1 blockade: In some cancers, the response to PD-1/PD-L1 blockades is independent of PD-L1 expression PD-L1 + p. show higher response and some PD-L1 - p. also reveal the response to PD-1/ PD-L1 inhs. Variability in methods and antibodies may lead to different results Clear definition for PD-L1 positivity is still not achieved Standardization of staining and scoring methods before PD-L1 widely used to predict response Expression is dynamic and heterogeneous due to changes of microenvironment or therapy Evaluation of PD-L1 at a single time point or single tumor may not predict the response to PD-1/PD-L1 inhs. PD-L1 does not seem a true patient selection biomarker up to now PD-L1 does not seem a solitary biomarker Blueprint Project
79 Our testing strategy could be improved, perhaps by additional markers or incorporation of some assessment of the immune cellular environment in the tumors, but a much greater quantity of validated data is required before our testing strategies can change Kerr KK, Arch Pathol Lab Med 2016
80
INMUNOTERAPIA EN EL CÁNCER DE PULMÓN 5 DE ABRIL DE 2017 DRA. BLANCA TRUJILLO R4 ONCOLOGÍA MÉDICA DRA. ÁLVAREZ CABELLOS
 INMUNOTERAPIA EN EL CÁNCER DE PULMÓN 5 DE ABRIL DE 2017 DRA. BLANCA TRUJILLO R4 ONCOLOGÍA MÉDICA DRA. ÁLVAREZ CABELLOS ESQUEMA DE LA SESIÓN 1. Introducción 2. Consideraciones generales del tratamiento
INMUNOTERAPIA EN EL CÁNCER DE PULMÓN 5 DE ABRIL DE 2017 DRA. BLANCA TRUJILLO R4 ONCOLOGÍA MÉDICA DRA. ÁLVAREZ CABELLOS ESQUEMA DE LA SESIÓN 1. Introducción 2. Consideraciones generales del tratamiento
Terapias anti PD1- PDL1. Luis de la Cruz Merino Sº Oncología Médica. HUVMacarena (Sevilla)
") Terapias anti PD1- PDL1 Luis de la Cruz Merino Sº Oncología Médica. HUVMacarena (Sevilla) INDICE EL EJE PD1/PD-L1 Y LA SINAPSIS INMUNE ANTICUERPOS MONOCLONALES EN ESTUDIO DESARROLLO AC MO ANTI PD1 EN MELANOMA
Terapias anti PD1- PDL1 Luis de la Cruz Merino Sº Oncología Médica. HUVMacarena (Sevilla) INDICE EL EJE PD1/PD-L1 Y LA SINAPSIS INMUNE ANTICUERPOS MONOCLONALES EN ESTUDIO DESARROLLO AC MO ANTI PD1 EN MELANOMA
OPTIMIZACIÓN TRATAMIENTO ANTI-EGFR. Ruth Vera Oncología Médica
 OPTIMIZACIÓN TRATAMIENTO ANTI-EGFR Ruth Vera Oncología Médica OPTIMIZACIÓN TRATAMIENTO anti-egfr OPTIMIZAR quiere decir: Buscar los mejores resultados Planificar una actividad para obtener los mejores
OPTIMIZACIÓN TRATAMIENTO ANTI-EGFR Ruth Vera Oncología Médica OPTIMIZACIÓN TRATAMIENTO anti-egfr OPTIMIZAR quiere decir: Buscar los mejores resultados Planificar una actividad para obtener los mejores
Cáncer de vejiga. Qué hemos aprendido estos últimos años? Begoña Mellado Hospital Clínic. Barcelona
 Cáncer de vejiga Qué hemos aprendido estos últimos años? Begoña Mellado Hospital Clínic. Barcelona Qué hemos aprendido estos últimos años de cáncer de vejiga? Tratamiento adyuvante/neoadyuvante Enfermedad
Cáncer de vejiga Qué hemos aprendido estos últimos años? Begoña Mellado Hospital Clínic. Barcelona Qué hemos aprendido estos últimos años de cáncer de vejiga? Tratamiento adyuvante/neoadyuvante Enfermedad
Cáncer de mama metastásico ER-/HER2+ y resistencia precoz a la terapia con trastuzumab
 Cáncer de mama metastásico ER-/HER2+ y resistencia precoz a la terapia con trastuzumab Eva M Ciruelos Gil Hospital Universitario 12 de Octubre, Madrid Caso clínico Paciente con cáncer de mama HER2+ y recidiva
Cáncer de mama metastásico ER-/HER2+ y resistencia precoz a la terapia con trastuzumab Eva M Ciruelos Gil Hospital Universitario 12 de Octubre, Madrid Caso clínico Paciente con cáncer de mama HER2+ y recidiva
Cáncer de vejiga avanzado: Quimioterapia en segunda línea y tratamiento de mantenimiento
 Cáncer de vejiga avanzado: Quimioterapia en segunda línea y tratamiento de mantenimiento Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Complutense University
Cáncer de vejiga avanzado: Quimioterapia en segunda línea y tratamiento de mantenimiento Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Complutense University
Terapia de campo de tumores en el tratamiento del glioblastoma
 Terapia de campo de tumores en el tratamiento del glioblastoma Revisión sistemática Informe de síntesis de tecnología emergente Tumor treating fields therapy (TTF) for glioblastoma. A Systematic Review
Terapia de campo de tumores en el tratamiento del glioblastoma Revisión sistemática Informe de síntesis de tecnología emergente Tumor treating fields therapy (TTF) for glioblastoma. A Systematic Review
RADIO-223 Y CÁNCER DE PRÓSTATA. ÁLVARO PINTO Servicio de Oncología Médica, Hospital La Paz
 RADIO-223 Y CÁNCER DE PRÓSTATA ÁLVARO PINTO Servicio de Oncología Médica, Hospital La Paz INTRODUCCIÓN METÁSTASIS ÓSEAS Prostate ~90% Myeloma 70-95%
RADIO-223 Y CÁNCER DE PRÓSTATA ÁLVARO PINTO Servicio de Oncología Médica, Hospital La Paz INTRODUCCIÓN METÁSTASIS ÓSEAS Prostate ~90% Myeloma 70-95%
LA EXPERIENCIA CLÍNICA COMO GARANTÍA DEL ÉXITO
 LA EXPERIENCIA CLÍNICA COMO GARANTÍA DEL ÉXITO Evaluación de la respuesta: Hasta cuando hay que mantener el tratamiento? ~ Dra. Ana Blasco Consorcio Hospital General Universitario de Valencia Dra. Virtudes
LA EXPERIENCIA CLÍNICA COMO GARANTÍA DEL ÉXITO Evaluación de la respuesta: Hasta cuando hay que mantener el tratamiento? ~ Dra. Ana Blasco Consorcio Hospital General Universitario de Valencia Dra. Virtudes
Evolución de la supervivencia en melanoma metastásico BRAF mutado. Nuevas estrategias de tratamiento.
 Evolución de la supervivencia en melanoma metastásico BRAF mutado. Nuevas estrategias de tratamiento. Dra. Ainara Soria Rivas Servicio de Oncología Médica Hospital Ramón y Cajal Cuál es la supervivencia
Evolución de la supervivencia en melanoma metastásico BRAF mutado. Nuevas estrategias de tratamiento. Dra. Ainara Soria Rivas Servicio de Oncología Médica Hospital Ramón y Cajal Cuál es la supervivencia
Cáncer de mama metastásico ER-/HER2+ y resistencia precoz a la terapia con trastuzumab
 Cáncer de mama metastásico ER-/HER2+ y resistencia precoz a la terapia con trastuzumab Eva M Ciruelos Gil Hospital Universitario 12 de Octubre, Madrid Caso clínico Paciente con cáncer de mama HER2+ y recidiva
Cáncer de mama metastásico ER-/HER2+ y resistencia precoz a la terapia con trastuzumab Eva M Ciruelos Gil Hospital Universitario 12 de Octubre, Madrid Caso clínico Paciente con cáncer de mama HER2+ y recidiva
Evaluación de respuesta: Hasta cuando hay que mantener el tratamiento? "
 Evaluación de respuesta: Hasta cuando hay que mantener el tratamiento? " Manuel Cobo Dols Oncologia Médica Hospital Universitario Málaga General y Virgen de la Victoria Cuestiones Cuál es la mejor forma
Evaluación de respuesta: Hasta cuando hay que mantener el tratamiento? " Manuel Cobo Dols Oncologia Médica Hospital Universitario Málaga General y Virgen de la Victoria Cuestiones Cuál es la mejor forma
Integrando la inmunoterapia en la práctica clínica en cáncer de pulmón no microcítico
 Integrando la inmunoterapia en la práctica clínica en cáncer de pulmón no microcítico Coordinador Científico: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla, Santander Organizado por:
Integrando la inmunoterapia en la práctica clínica en cáncer de pulmón no microcítico Coordinador Científico: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla, Santander Organizado por:
INMUNOTERAPIA EN CÁNCER DE CABEZA Y CUELLO. JULIO LAMBEA SORROSAL Servicio de Oncología Médica CLÍNICO LOZANO BLESA ZARAGOZA
 INMUNOTERAPIA EN CÁNCER DE CABEZA Y CUELLO JULIO LAMBEA SORROSAL Servicio de Oncología Médica CLÍNICO LOZANO BLESA ZARAGOZA HISTORIA DEL TRATAMIENTO DE LOS TUMORES DE CABEZA Y CUELLO 2 HISTORIA DEL TRATAMIENTO
INMUNOTERAPIA EN CÁNCER DE CABEZA Y CUELLO JULIO LAMBEA SORROSAL Servicio de Oncología Médica CLÍNICO LOZANO BLESA ZARAGOZA HISTORIA DEL TRATAMIENTO DE LOS TUMORES DE CABEZA Y CUELLO 2 HISTORIA DEL TRATAMIENTO
TUMORES DE CABEZA Y CUELLO RECURRENTES /METASTÁSICOS A FAVOR DE LA INMUNOTERAPIA
 TUMORES DE CABEZA Y CUELLO RECURRENTES /METASTÁSICOS A FAVOR DE LA INMUNOTERAPIA JULIO LAMBEA SORROSAL Servicio de Oncología Médica CLÍNICO LOZANO BLESA ZARAGOZA 1 HISTORIA DEL TRATAMIENTO DE LOS TUMORES
TUMORES DE CABEZA Y CUELLO RECURRENTES /METASTÁSICOS A FAVOR DE LA INMUNOTERAPIA JULIO LAMBEA SORROSAL Servicio de Oncología Médica CLÍNICO LOZANO BLESA ZARAGOZA 1 HISTORIA DEL TRATAMIENTO DE LOS TUMORES
Qué hacemos con los pacientes B-RAF mutados? Alfonso Berrocal Hospital General Universitario, Valencia
 Qué hacemos con los pacientes B-RAF mutados? Alfonso Berrocal Hospital General Universitario, Valencia Ventajas y desventajas de la inmunoterapia Ventajas Pacientes Largos supervivientes Ipilimumab 20%
Qué hacemos con los pacientes B-RAF mutados? Alfonso Berrocal Hospital General Universitario, Valencia Ventajas y desventajas de la inmunoterapia Ventajas Pacientes Largos supervivientes Ipilimumab 20%
ESQUEMAS ALTERNATIVOS CON SUNITINIB: MÁS ALLÁ DEL MANEJO DE LOS EFECTOS ADVERSOS
 ESQUEMAS ALTERNATIVOS CON SUNITINIB: MÁS ALLÁ DEL MANEJO DE LOS EFECTOS ADVERSOS María Jose Lecumberri Biurrun CHN León, 20 de mayo de 2016 Estudio fase III de sunitinib vs interferón alfa en primera línea
ESQUEMAS ALTERNATIVOS CON SUNITINIB: MÁS ALLÁ DEL MANEJO DE LOS EFECTOS ADVERSOS María Jose Lecumberri Biurrun CHN León, 20 de mayo de 2016 Estudio fase III de sunitinib vs interferón alfa en primera línea
Investigación Translacional en Farmacoterapia
 Investigación Translacional en Farmacoterapia Eloisa Jantus Lewintre Laboratorio Oncología Molecular Servicio Oncología Médica Dpto Biotecnología CIBERONC Investigación traslacional Qué? Dónde? Cómo? Investigación
Investigación Translacional en Farmacoterapia Eloisa Jantus Lewintre Laboratorio Oncología Molecular Servicio Oncología Médica Dpto Biotecnología CIBERONC Investigación traslacional Qué? Dónde? Cómo? Investigación
Estrategias de inmunoterapia en cáncer genitourinario
 Estrategias de inmunoterapia en cáncer genitourinario Iván Martínez Forero MD, PhD Hospital Pablo Tobón Uribe imforero@hptu.org.co imforero@alumni.unav.es Disclosure BMS-Speaker Contenido Respuesta inmune
Estrategias de inmunoterapia en cáncer genitourinario Iván Martínez Forero MD, PhD Hospital Pablo Tobón Uribe imforero@hptu.org.co imforero@alumni.unav.es Disclosure BMS-Speaker Contenido Respuesta inmune
ALTERNATIVAS: 2ª Línea y posteriores. Dra. Ruth Vera Servicio Oncología Médica Complejo Hospitalario de Navarra
 ALTERNATIVAS: 2ª Línea y posteriores Dra. Ruth Vera Servicio Oncología Médica Complejo Hospitalario de Navarra 1. INTRODUCCIÓN 2. TRATAMIENTO DE SEGUNDA LÍNEA CON TERAPIAS ANTIEGFR 1. TRATAMIENTO DE SEGUNDA
ALTERNATIVAS: 2ª Línea y posteriores Dra. Ruth Vera Servicio Oncología Médica Complejo Hospitalario de Navarra 1. INTRODUCCIÓN 2. TRATAMIENTO DE SEGUNDA LÍNEA CON TERAPIAS ANTIEGFR 1. TRATAMIENTO DE SEGUNDA
Club de Inmunohistoquímica y Biología Molecular. Mª Dolores Lozano Escario Clínica Universidad de Navarra. Pamplona.
 Club de Inmunohistoquímica y Biología Molecular Mª Dolores Lozano Escario Clínica Universidad de Navarra. Pamplona. Cuando me invitan a dar charlas un poco filosóficas pienso que mi vida profesional está
Club de Inmunohistoquímica y Biología Molecular Mª Dolores Lozano Escario Clínica Universidad de Navarra. Pamplona. Cuando me invitan a dar charlas un poco filosóficas pienso que mi vida profesional está
Diagnóstico actual del cáncer pulmonar: rol de EBUS-TBNA desde la perspectiva del Anátomo-Patólogo.
 Diagnóstico actual del cáncer pulmonar: rol de EBUS-TBNA desde la perspectiva del Anátomo-Patólogo. Dra. Yumay Pires N. Servicio de Anatomía Patológica Clinica Alemana 12,9% del total de nuevos casos de
Diagnóstico actual del cáncer pulmonar: rol de EBUS-TBNA desde la perspectiva del Anátomo-Patólogo. Dra. Yumay Pires N. Servicio de Anatomía Patológica Clinica Alemana 12,9% del total de nuevos casos de
PATOLOGIA MOLECULAR DEL CARCINOMA DE COLON. Eva Musulén
 PATOLOGIA MOLECULAR DEL CARCINOMA DE COLON Eva Musulén Patología molecular del CCR 1. Identificar pacientes de riesgo (Síndrome de Lynch) Inestabilidad de microsatélites 2. Guiar estrategia terapéutica
PATOLOGIA MOLECULAR DEL CARCINOMA DE COLON Eva Musulén Patología molecular del CCR 1. Identificar pacientes de riesgo (Síndrome de Lynch) Inestabilidad de microsatélites 2. Guiar estrategia terapéutica
Base de Datos Carcinoides Bronquiales
 Base de Datos Carcinoides Bronquiales Justificación Neoplasias de estirpe neuroendocrina y asiento pulmonar Yao JC, et al. J Clin Oncol 2008:26;3063-3072 Justificación 35.825 casos (1973-2004) % Primario
Base de Datos Carcinoides Bronquiales Justificación Neoplasias de estirpe neuroendocrina y asiento pulmonar Yao JC, et al. J Clin Oncol 2008:26;3063-3072 Justificación 35.825 casos (1973-2004) % Primario
Biopsia Liquida Utilidad Clínica- Impacto en la Oncología
 The changing face of cancer diagnosis Biopsia Liquida Utilidad Clínica- Impacto en la Oncología Carlos Camps H. General Universitario Valencia Guía de la Ponencia Peculiaridades del Cáncer Peculiaridades
The changing face of cancer diagnosis Biopsia Liquida Utilidad Clínica- Impacto en la Oncología Carlos Camps H. General Universitario Valencia Guía de la Ponencia Peculiaridades del Cáncer Peculiaridades
Cómo definen los Oncólogos Alta Carga Tumoral en Cáncer de Mama Metastásico?
 Cómo definen los Oncólogos Alta Carga Tumoral en Cáncer de Mama Metastásico? Consenso sobre Cáncer de Mama Agresivo Her2- en Primera línea de Quimioterapia Consenso sobre Cáncer de Mama Agresivo Her2-
Cómo definen los Oncólogos Alta Carga Tumoral en Cáncer de Mama Metastásico? Consenso sobre Cáncer de Mama Agresivo Her2- en Primera línea de Quimioterapia Consenso sobre Cáncer de Mama Agresivo Her2-
Caso clínico 4: Paciente joven luminal con enfermedad ósea. Dra. Ana Lluch Hospital Clínico Universitariode Valencia
 Caso clínico 4: Paciente joven luminal con enfermedad ósea Dra. Ana Lluch Hospital Clínico Universitariode Valencia El contenido de esta presentación refleja las opiniones, criterios, conclusiones y/o
Caso clínico 4: Paciente joven luminal con enfermedad ósea Dra. Ana Lluch Hospital Clínico Universitariode Valencia El contenido de esta presentación refleja las opiniones, criterios, conclusiones y/o
En esta primera sesión de comunicaciones orales sobre melanoma y otros tumores cutáneos se han presentado las siguientes comunicaciones:
 En esta primera sesión de comunicaciones orales sobre se han presentado las siguientes comunicaciones: 1213O. Characterization of complete responses (CRs) in patients with advanced melanoma (MEL) who received
En esta primera sesión de comunicaciones orales sobre se han presentado las siguientes comunicaciones: 1213O. Characterization of complete responses (CRs) in patients with advanced melanoma (MEL) who received
El Inmunomomento en Melanoma: Nivolumab más respuestas y larga supervivencia? Alfonso Berrocal
 El Inmunomomento en Melanoma: Nivolumab más respuestas y larga supervivencia? Alfonso Berrocal Proporción vivos Supervivencia con Ipilumumab en acceso expandido 1.0 0.9 0.8 Mediana de supervivencia meses
El Inmunomomento en Melanoma: Nivolumab más respuestas y larga supervivencia? Alfonso Berrocal Proporción vivos Supervivencia con Ipilumumab en acceso expandido 1.0 0.9 0.8 Mediana de supervivencia meses
Quimioterapia en Cáncer de Vejiga. Dr. Ovidio Fernández Calvo Complejo Hospitalario Universitario Ourense
 Quimioterapia en Cáncer de Vejiga Dr. Ovidio Fernández Calvo Complejo Hospitalario Universitario Ourense Evolution of systemic therapy for urothelial cancer 1 Sternberg CN et al. Cancer 1989;64(12):2448
Quimioterapia en Cáncer de Vejiga Dr. Ovidio Fernández Calvo Complejo Hospitalario Universitario Ourense Evolution of systemic therapy for urothelial cancer 1 Sternberg CN et al. Cancer 1989;64(12):2448
ESTUDIO DE BIOMARCADORES Y VALOR CLÍNICO DE LA BIOPSIA LÍQUIDA EN MELANOMA
 ESTUDIO DE BIOMARCADORES Y VALOR CLÍNICO DE LA BIOPSIA LÍQUIDA EN MELANOMA José Luis Rodríguez Peralto HOSPITAL 12 DE OCTUBRE, MADRID GENOMIC CHANGES IN THE NUMBER OF DNA COPIES IN DIFFERENTS SUBTYPES
ESTUDIO DE BIOMARCADORES Y VALOR CLÍNICO DE LA BIOPSIA LÍQUIDA EN MELANOMA José Luis Rodríguez Peralto HOSPITAL 12 DE OCTUBRE, MADRID GENOMIC CHANGES IN THE NUMBER OF DNA COPIES IN DIFFERENTS SUBTYPES
INFORME 2: Sesión general de pósters sobre melanoma PARTE I - Chicago, sábado 3 de junio de 2017
 A continuación, destacamos los hallazgos más relevantes de pósters de ASCO en melanoma agrupados en los siguientes temas: Combinaciones de inmunoterapia Neoadyuvancia Otros 1 - Combinaciones de inmunoterapia
A continuación, destacamos los hallazgos más relevantes de pósters de ASCO en melanoma agrupados en los siguientes temas: Combinaciones de inmunoterapia Neoadyuvancia Otros 1 - Combinaciones de inmunoterapia
Guión de la presentación
 Actualización en biomarcadores y guía de recomendación en el cáncer de mama Curso de Biomarcadores XXVI Congreso Nacional de la SEAP Federico Rojo Fundación Jiménez Díaz Guión de la presentación Quédebemos
Actualización en biomarcadores y guía de recomendación en el cáncer de mama Curso de Biomarcadores XXVI Congreso Nacional de la SEAP Federico Rojo Fundación Jiménez Díaz Guión de la presentación Quédebemos
José Luis Pérez Gracia Departamento de Oncología Clínica Universidad de Navarra Madrid, 20 de noviembre de 2014
 Inmunoterapia en cáncer renal y futuro de las combinaciones con TKI José Luis Pérez Gracia Departamento de Oncología Clínica Universidad de Navarra Madrid, 20 de noviembre de 2014 Steps leading to an anti
Inmunoterapia en cáncer renal y futuro de las combinaciones con TKI José Luis Pérez Gracia Departamento de Oncología Clínica Universidad de Navarra Madrid, 20 de noviembre de 2014 Steps leading to an anti
Conclusiones Cáncer ginecológico
 Conclusiones Cáncer ginecológico Conclusiones Cáncer ginecológico ONCO NEXT GEN Inmunoterapia Recaída tardía Sin mbrca QT intraperitoneal A favor Conclusiones Cáncer ginecológico ONCOSAURIOS ONCO SENIOR
Conclusiones Cáncer ginecológico Conclusiones Cáncer ginecológico ONCO NEXT GEN Inmunoterapia Recaída tardía Sin mbrca QT intraperitoneal A favor Conclusiones Cáncer ginecológico ONCOSAURIOS ONCO SENIOR
Alternativas de tratamiento de segunda línea postdocetaxel en Cáncer de Próstata en progresión con niveles de castración de testosterona (CPRC)
") Alternativas de tratamiento de segunda línea postdocetaxel en Cáncer de Próstata en progresión con niveles de castración de testosterona (CPRC) Dr Pablo Maroto Oncología Médica, Hospital de Sant Pau El
Alternativas de tratamiento de segunda línea postdocetaxel en Cáncer de Próstata en progresión con niveles de castración de testosterona (CPRC) Dr Pablo Maroto Oncología Médica, Hospital de Sant Pau El
Fernando Henao Carrasco Hospital Virgen Macarena Sevilla.
 Inmunoterapia vs terapias dirigidas: optimización de tratamiento, secuenciación y mantenimiento. Ensayos clínicos al respecto Fernando Henao Carrasco Hospital Virgen Macarena Sevilla. Indice Introducción
Inmunoterapia vs terapias dirigidas: optimización de tratamiento, secuenciación y mantenimiento. Ensayos clínicos al respecto Fernando Henao Carrasco Hospital Virgen Macarena Sevilla. Indice Introducción
Cáncer colorrectal metastático cómo decidir la mejor secuencia de tratamiento? Cristina Grávalos Hospital Universitario Marqués de Valdecilla
 Cáncer colorrectal metastático cómo decidir la mejor secuencia de tratamiento? Cristina Grávalos Hospital Universitario Marqués de Valdecilla Introducción - Cáncer colorrectal en España en el año 2012
Cáncer colorrectal metastático cómo decidir la mejor secuencia de tratamiento? Cristina Grávalos Hospital Universitario Marqués de Valdecilla Introducción - Cáncer colorrectal en España en el año 2012
Avances y Retos en Oncologica. Manuel Hidalgo, M.D., Ph.D.
 Avances y Retos en Oncologica Manuel Hidalgo, M.D., Ph.D. Agenda Conocimiento basico. Prevencion. Diagnostico. Tratamiento. The Hallmarks of Cancer Hanahan and Weinberg, Cell 2000 Simplified view of EGFR
Avances y Retos en Oncologica Manuel Hidalgo, M.D., Ph.D. Agenda Conocimiento basico. Prevencion. Diagnostico. Tratamiento. The Hallmarks of Cancer Hanahan and Weinberg, Cell 2000 Simplified view of EGFR
CANCER UNKNOWN PRIMARY
 CANCER UNKNOWN PRIMARY 3-5 % of diagnosed cancers Variability depending of centers 50% adenocarcinomas Immunohistochemistry helps in 30-85% Gene expression assays help in 75-90% Both methods solve > 95%
CANCER UNKNOWN PRIMARY 3-5 % of diagnosed cancers Variability depending of centers 50% adenocarcinomas Immunohistochemistry helps in 30-85% Gene expression assays help in 75-90% Both methods solve > 95%
Tratamiento inmunoterápico de las metástasis cerebrales. Alfonso Berrocal Hospital General de Valencia
 Tratamiento inmunoterápico de las metástasis cerebrales Alfonso Berrocal Hospital General de Valencia Inmunidad y metástasis cerebrales Cancer 2013;119:2737-46. Ipilimumab y metástasis SNC Ipilimumab bloquea
Tratamiento inmunoterápico de las metástasis cerebrales Alfonso Berrocal Hospital General de Valencia Inmunidad y metástasis cerebrales Cancer 2013;119:2737-46. Ipilimumab y metástasis SNC Ipilimumab bloquea
Novedad en el tratamiento del cáncer diferenciado de tiroides: Lenvatinib. Dra. T. Ramón y Cajal Hospital Sant Pau
 Novedad en el tratamiento del cáncer diferenciado de tiroides: Lenvatinib Dra. T. Ramón y Cajal Hospital Sant Pau Incidencia y mortalidad Incidencia creciente 12ª causa tumor sólido mujer 17ª causa tumor
Novedad en el tratamiento del cáncer diferenciado de tiroides: Lenvatinib Dra. T. Ramón y Cajal Hospital Sant Pau Incidencia y mortalidad Incidencia creciente 12ª causa tumor sólido mujer 17ª causa tumor
Qué hay de nuevo en el tratamiento del Cáncer de Vejiga? Guillermo Crespo Herrero Hospital Universitario de Burgos
 Qué hay de nuevo en el tratamiento del Cáncer de Vejiga? Guillermo Crespo Herrero Hospital Universitario de Burgos Coordinador Científico: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla,
Qué hay de nuevo en el tratamiento del Cáncer de Vejiga? Guillermo Crespo Herrero Hospital Universitario de Burgos Coordinador Científico: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla,
NOVETATS EN EL MANEIG DE LES DISLIPIDÈMIES: LDL molt baix. Hi ha corba J? Aporta beneficis?
 NOVETATS EN EL MANEIG DE LES DISLIPIDÈMIES: LDL molt baix. Hi ha corba J? Aporta beneficis? LUIS MASANA Unidad de Medicina Vascular y Metabolismo Hospital Universitario Sant Joan Universitat Rovira i Virgili
NOVETATS EN EL MANEIG DE LES DISLIPIDÈMIES: LDL molt baix. Hi ha corba J? Aporta beneficis? LUIS MASANA Unidad de Medicina Vascular y Metabolismo Hospital Universitario Sant Joan Universitat Rovira i Virgili
Respiratory Tract Tumors Program Red Temática de Investigación Cooperativa en Cáncer (RTICC)
") Respiratory Tract Tumors Program Red Temática de Investigación Cooperativa en Cáncer (RTICC) J.L. González Larriba Servicio de Oncologia Médica Hospital Clínico San Carlos Reunión 7 de Marzo 2013. Madrid.
Respiratory Tract Tumors Program Red Temática de Investigación Cooperativa en Cáncer (RTICC) J.L. González Larriba Servicio de Oncologia Médica Hospital Clínico San Carlos Reunión 7 de Marzo 2013. Madrid.
Farmacogenética y Farmacogenómica. Su aplicación en la gestión clínica diaria.
 Farmacogenética y Farmacogenómica. Su aplicación en la gestión clínica diaria. Montserrat Baiget Servicio de Genética Hospital de la Santa Creu i Sant Pau Barcelona EMA (European Medicines Agency) Genomic
Farmacogenética y Farmacogenómica. Su aplicación en la gestión clínica diaria. Montserrat Baiget Servicio de Genética Hospital de la Santa Creu i Sant Pau Barcelona EMA (European Medicines Agency) Genomic
Derechos reservados AVL, JADD, AJBG, queda prohibida su reproducción total y/o parcial.
 FAILURE THEORIES (From Shigley s Mechanical Engineering Design) MSS theory is an acceptable but conservative predictor of failure; and since engineers are conservative by nature, it is quite often used.
FAILURE THEORIES (From Shigley s Mechanical Engineering Design) MSS theory is an acceptable but conservative predictor of failure; and since engineers are conservative by nature, it is quite often used.
Detección del Ganglio Centinela en Patología Abdominal. Dra. C Balagué
 Detección del Ganglio Centinela en Patología Abdominal Dra. C Balagué DISEMINACIÓN LINFÁTICA Patrón ordenado, secuencial y predecible a través de los conductos linfáticos. GANGLIO CENTINELA Ganglios con
Detección del Ganglio Centinela en Patología Abdominal Dra. C Balagué DISEMINACIÓN LINFÁTICA Patrón ordenado, secuencial y predecible a través de los conductos linfáticos. GANGLIO CENTINELA Ganglios con
Experiencia con Vinorelbina Oral en el tratamiento del CPNM con histología no escamoso. Dr. Javier de Castro
 Experiencia con Vinorelbina Oral en el tratamiento del CPNM con histología no escamoso Dr. Javier de Castro Caso Clínico: carcinoma de pulmón no escamoso avanzado Mujer de 60 años Fumadora de 30 cig/d
Experiencia con Vinorelbina Oral en el tratamiento del CPNM con histología no escamoso Dr. Javier de Castro Caso Clínico: carcinoma de pulmón no escamoso avanzado Mujer de 60 años Fumadora de 30 cig/d
Fe Viva: Lo que sucede cuando la fe verdadera enciende las vidas del pueblo de Dios (Spanish Edition)
") Fe Viva: Lo que sucede cuando la fe verdadera enciende las vidas del pueblo de Dios (Spanish Edition) Click here if your download doesn"t start automatically Fe Viva: Lo que sucede cuando la fe verdadera
Fe Viva: Lo que sucede cuando la fe verdadera enciende las vidas del pueblo de Dios (Spanish Edition) Click here if your download doesn"t start automatically Fe Viva: Lo que sucede cuando la fe verdadera
Grupo Español Multidisciplinar en Cáncer Digestivo (GEMCAD)
") Grupo Español Multidisciplinar en Cáncer Digestivo (GEMCAD) GRUPO ESPAÑOL MULTIDISCIPLINAR EN CÁNCER DIGESTIVO Mail: secretaría@gemcad.org Telf. Contacto: 93 434 44 12 Presidente: Dr. Joan Maurel Santasusana
Grupo Español Multidisciplinar en Cáncer Digestivo (GEMCAD) GRUPO ESPAÑOL MULTIDISCIPLINAR EN CÁNCER DIGESTIVO Mail: secretaría@gemcad.org Telf. Contacto: 93 434 44 12 Presidente: Dr. Joan Maurel Santasusana
TRATAMIENTO DE LOS CARCINOMAS NEUROENDOCRINOS. Guillermo Crespo Herrero Oncología Médica Hospital Universitario de Burgos
 TRATAMIENTO DE LOS CARCINOMAS NEUROENDOCRINOS Guillermo Crespo Herrero Oncología Médica Hospital Universitario de Burgos CNE G3 CÉLULA PEQUEÑA KI67 70% ORIGEN DESCONOCIDO DIC-13 CARBOPLATINO ETOPOSIDO
TRATAMIENTO DE LOS CARCINOMAS NEUROENDOCRINOS Guillermo Crespo Herrero Oncología Médica Hospital Universitario de Burgos CNE G3 CÉLULA PEQUEÑA KI67 70% ORIGEN DESCONOCIDO DIC-13 CARBOPLATINO ETOPOSIDO
Terapias anti CTLA-4. Curso Básico de Inmunología e Inmunoterapia y cáncer. Alfonso Berrocal Hospital General Valencia
 Terapias anti CTLA-4 Curso Básico de Inmunología e Inmunoterapia y cáncer Alfonso Berrocal Hospital General Valencia Mecanismo de acción Teoría Tres señales: Co-estimulación Interacción B7/CD28 CD28 se
Terapias anti CTLA-4 Curso Básico de Inmunología e Inmunoterapia y cáncer Alfonso Berrocal Hospital General Valencia Mecanismo de acción Teoría Tres señales: Co-estimulación Interacción B7/CD28 CD28 se
A propósito de un caso: metástasis cerebrales de melanoma ASUNCIÓN JUÁREZ MARROQUÍ HOSPITAL DE ELDA
 A propósito de un caso: metástasis cerebrales de melanoma ASUNCIÓN JUÁREZ MARROQUÍ HOSPITAL DE ELDA Caso clínico Mujer 54 años Septiembre 2013 (Cl. Privada): Exéresis de lunar región trapezoide (no AP).
A propósito de un caso: metástasis cerebrales de melanoma ASUNCIÓN JUÁREZ MARROQUÍ HOSPITAL DE ELDA Caso clínico Mujer 54 años Septiembre 2013 (Cl. Privada): Exéresis de lunar región trapezoide (no AP).
Inmunoterapia del Melanoma Maligno: Rompiendo Barreras. Alfonso Berrocal Servicio Oncología Medica Hospital General de Valencia
 Inmunoterapia del Melanoma Maligno: Rompiendo Barreras Alfonso Berrocal Servicio Oncología Medica Hospital General de Valencia Avances por mejor conocimiento de la biología McArthur GA, Ribas A. J Clin
Inmunoterapia del Melanoma Maligno: Rompiendo Barreras Alfonso Berrocal Servicio Oncología Medica Hospital General de Valencia Avances por mejor conocimiento de la biología McArthur GA, Ribas A. J Clin
CÁNCER DE MAMA: TRATAMIENTO NEOADYUVANTE Triple Negativo. César A. Rodríguez Hospital Universitario de Salamanca
 CÁNCER DE MAMA: TRATAMIENTO NEOADYUVANTE Triple Negativo César A. Rodríguez Hospital Universitario de Salamanca Introducción 60 pcr Rates by Tumor Subtypes 50 40 50 30 20 30 31. 34 10 16 18 7 0 Grade 1-2
CÁNCER DE MAMA: TRATAMIENTO NEOADYUVANTE Triple Negativo César A. Rodríguez Hospital Universitario de Salamanca Introducción 60 pcr Rates by Tumor Subtypes 50 40 50 30 20 30 31. 34 10 16 18 7 0 Grade 1-2
Cáncer de Mama: Inhibidores de vía PI3K/Akt/mTOR, ciclinas, anti-ctla4 y anti PD1. Dr. Claudio Painemal D. Director Médico
 Cáncer de Mama: Inhibidores de vía PI3K/Akt/mTOR, ciclinas, anti-ctla4 y anti PD1 Dr. Claudio Painemal D. Director Médico PI3K/Akt/mTOR Frecuentemente activada en cáncer de mama PIK3CA es el gen más frecuentemente
Cáncer de Mama: Inhibidores de vía PI3K/Akt/mTOR, ciclinas, anti-ctla4 y anti PD1 Dr. Claudio Painemal D. Director Médico PI3K/Akt/mTOR Frecuentemente activada en cáncer de mama PIK3CA es el gen más frecuentemente
Innovación terapéutica en cáncer de pulmón. Dr A. Artal Hospital Universitario Miguel Servet Zaragoza
 Innovación terapéutica en cáncer de pulmón Dr A. Artal Hospital Universitario Miguel Servet Zaragoza NINTEDANIB INMUNOTERAPIA NINTEDANIB INMUNOTERAPIA Second line First line Study Intervention Target PFS,
Innovación terapéutica en cáncer de pulmón Dr A. Artal Hospital Universitario Miguel Servet Zaragoza NINTEDANIB INMUNOTERAPIA NINTEDANIB INMUNOTERAPIA Second line First line Study Intervention Target PFS,
Futuro de las combinaciones (de inmunoterapia) en el tratamiento del melanoma avanzado
 en el tratamiento del melanoma avanzado") Futuro de las combinaciones (de inmunoterapia) en el tratamiento del melanoma avanzado Iván Márquez Rodas MD, PhD Servicio de Oncología Médica Hospital General Universitario Gregorio Marañón DISCLOSURES
Futuro de las combinaciones (de inmunoterapia) en el tratamiento del melanoma avanzado Iván Márquez Rodas MD, PhD Servicio de Oncología Médica Hospital General Universitario Gregorio Marañón DISCLOSURES
RELACIÓN ENTRE LOS NIVELES DE CREATINA CINASA MB Y TROPONINA I CON EL ESTADIO DE ENFERMEDAD RENAL CRÓNICA, CIUDAD HOSPITALARIA DR. ENRIQUE TEJERA.
 RELACIÓN ENTRE LOS NIVELES DE CREATINA CINASA MB Y TROPONINA I CON EL ESTADIO DE ENFERMEDAD RENAL CRÓNICA, CIUDAD HOSPITALARIA DR. ENRIQUE TEJERA. ENERO-MAYO 2015 ii UNIVERSIDAD DE CARABOBO FACULTAD DE
RELACIÓN ENTRE LOS NIVELES DE CREATINA CINASA MB Y TROPONINA I CON EL ESTADIO DE ENFERMEDAD RENAL CRÓNICA, CIUDAD HOSPITALARIA DR. ENRIQUE TEJERA. ENERO-MAYO 2015 ii UNIVERSIDAD DE CARABOBO FACULTAD DE
Mujer con cáncer de mama y
 Mujer con cáncer de mama y Oliver Higuera Gómez R4 Oncología Médica H.U. La Paz Antecedentes personales Mujer de 48 años de edad No reacciones alérgicas medicamentosas conocidas Fiebre reumática en la
Mujer con cáncer de mama y Oliver Higuera Gómez R4 Oncología Médica H.U. La Paz Antecedentes personales Mujer de 48 años de edad No reacciones alérgicas medicamentosas conocidas Fiebre reumática en la
El Jardín de la Memoria (El adepto de la Reina nº 2) (Spanish Edition)
 (Spanish Edition)") El Jardín de la Memoria (El adepto de la Reina nº 2) (Spanish Edition) Rodolfo Martínez Click here if your download doesn"t start automatically Download and Read Free Online El Jardín de la Memoria (El
El Jardín de la Memoria (El adepto de la Reina nº 2) (Spanish Edition) Rodolfo Martínez Click here if your download doesn"t start automatically Download and Read Free Online El Jardín de la Memoria (El
REDEFINIENDO EL PAPEL DE LA QUIMIOTERAPIA EN CÁNCER DE MAMA METASTÁSICO. Jesús García Mata C.H.U.Ourense
 REDEFINIENDO EL PAPEL DE LA QUIMIOTERAPIA EN CÁNCER DE MAMA METASTÁSICO Jesús García Mata C.H.U.Ourense Tto.Sistémico Hormonoterapia Tto. Biológico Quimioterapia Fenotipos Cáncer de Mama RE+ 65% 75% Cáncer
REDEFINIENDO EL PAPEL DE LA QUIMIOTERAPIA EN CÁNCER DE MAMA METASTÁSICO Jesús García Mata C.H.U.Ourense Tto.Sistémico Hormonoterapia Tto. Biológico Quimioterapia Fenotipos Cáncer de Mama RE+ 65% 75% Cáncer
MANUAL DE FARMACIA CLINICA Y ATENCION FARMACEUTICA. EL PRECIO ES EN DOLARES BY JOAQUIN HERRERA CARRANZA
 MANUAL DE FARMACIA CLINICA Y ATENCION FARMACEUTICA. EL PRECIO ES EN DOLARES BY JOAQUIN HERRERA CARRANZA DOWNLOAD EBOOK : MANUAL DE FARMACIA CLINICA Y ATENCION HERRERA CARRANZA PDF Click link bellow and
MANUAL DE FARMACIA CLINICA Y ATENCION FARMACEUTICA. EL PRECIO ES EN DOLARES BY JOAQUIN HERRERA CARRANZA DOWNLOAD EBOOK : MANUAL DE FARMACIA CLINICA Y ATENCION HERRERA CARRANZA PDF Click link bellow and
XX JORNADA DE LA SOCIEDAD DE MEDICINA NUCLEAR E IMAGEN MOLECULAR DE VALENCIA Y MURCIA
 XX JORNADA DE LA SOCIEDAD DE MEDICINA NUCLEAR E IMAGEN MOLECULAR DE VALENCIA Y MURCIA Dra Virtudes Soriano Fundación Instituto Valenciano de Oncologia Valencia 29 de Abril 2016 HISTORIA INMUNOTERAPIA EN
XX JORNADA DE LA SOCIEDAD DE MEDICINA NUCLEAR E IMAGEN MOLECULAR DE VALENCIA Y MURCIA Dra Virtudes Soriano Fundación Instituto Valenciano de Oncologia Valencia 29 de Abril 2016 HISTORIA INMUNOTERAPIA EN
MENSAJES PARA LLEVARSE A CASA MESA 7: CANCER DE PULMON Y GENITO-URINARIO LOURDES CALERA HOSPITAL SIERRALLANA
 MENSAJES PARA LLEVARSE A CASA MESA 7: CANCER DE PULMON Y GENITO-URINARIO LOURDES CALERA HOSPITAL SIERRALLANA MENSAJES PARA LLEVARSE A CASA: INNOVACIONES EN EL TRATAMIENTO DEL CANCER RENAL QUE HAY DE NUEVO
MENSAJES PARA LLEVARSE A CASA MESA 7: CANCER DE PULMON Y GENITO-URINARIO LOURDES CALERA HOSPITAL SIERRALLANA MENSAJES PARA LLEVARSE A CASA: INNOVACIONES EN EL TRATAMIENTO DEL CANCER RENAL QUE HAY DE NUEVO
Efectividad de la automonitorización y autocontrol del tratamiento con anticoagulantes orales antagonistas de la vitamina K
 Efectividad de la automonitorización y autocontrol del tratamiento con anticoagulantes orales antagonistas de la vitamina K Revisión sistemática Effectiveness of patient self-testing and patient self-management
Efectividad de la automonitorización y autocontrol del tratamiento con anticoagulantes orales antagonistas de la vitamina K Revisión sistemática Effectiveness of patient self-testing and patient self-management
CONTROLADORA PARA PIXELS CONPIX
 The LedEdit Software Instructions 1, Install the software to PC and open English version: When we installed The LedEdit Software, on the desktop we can see following icon: Please Double-click it, then
The LedEdit Software Instructions 1, Install the software to PC and open English version: When we installed The LedEdit Software, on the desktop we can see following icon: Please Double-click it, then
CÁNCER GÁSTRICO AVANZADO: ALTERNATIVAS EN SEGUNDA LÍNEA. Fernando Rivera Herrero Sv Oncología Médica HU M Valdecilla. Santander
 CÁNCER GÁSTRICO AVANZADO: ALTERNATIVAS EN SEGUNDA LÍNEA Fernando Rivera Herrero Sv Oncología Médica HU M Valdecilla. Santander Cáncer Gástrico Avanzado: alternativas en 2ª línea Varios estándares en 1ª
CÁNCER GÁSTRICO AVANZADO: ALTERNATIVAS EN SEGUNDA LÍNEA Fernando Rivera Herrero Sv Oncología Médica HU M Valdecilla. Santander Cáncer Gástrico Avanzado: alternativas en 2ª línea Varios estándares en 1ª
ESTUDIO OBINDIAB GRUPO DE DIABETES SEMFYC
 ESTUDIO OBINDIAB GRUPO DE DIABETES SEMFYC METHODS CHARACTERISTICS OF THE PATIENTS Mean (SD) Range CI95% Age (years) 68,9+11,3 40-95 (67,8-70,0) HbA1c (%) 6,97+1,2 5,0-14,7 (6,9-7,1) Gender Male Female
ESTUDIO OBINDIAB GRUPO DE DIABETES SEMFYC METHODS CHARACTERISTICS OF THE PATIENTS Mean (SD) Range CI95% Age (years) 68,9+11,3 40-95 (67,8-70,0) HbA1c (%) 6,97+1,2 5,0-14,7 (6,9-7,1) Gender Male Female
Nuevas Estrategias con Inhibidores de Puntos de Control Celular en Linfomas de Hodgkin
 Nuevas Estrategias con Inhibidores de Puntos de Control Celular en Linfomas de Hodgkin Dra. María Alejandra Torres Viera Hematología Oncología 360, Caracas Caracas, Marzo 2016!" LH: Sobrevida De Acuerdo
Nuevas Estrategias con Inhibidores de Puntos de Control Celular en Linfomas de Hodgkin Dra. María Alejandra Torres Viera Hematología Oncología 360, Caracas Caracas, Marzo 2016!" LH: Sobrevida De Acuerdo
EVALUACIÓN DE RESULTADOS DE CRIZOTINIB EN CÁNCER DE PULMÓN NO MICROCÍTICO. Mª José Moreno Fernández
 EVALUACIÓN DE RESULTADOS DE CRIZOTINIB EN CÁNCER DE PULMÓN NO MICROCÍTICO Mª José Moreno Fernández Introducción. Situación actual de Crizotinib. Objetivos. Material y métodos. Resultados. Limitaciones
EVALUACIÓN DE RESULTADOS DE CRIZOTINIB EN CÁNCER DE PULMÓN NO MICROCÍTICO Mª José Moreno Fernández Introducción. Situación actual de Crizotinib. Objetivos. Material y métodos. Resultados. Limitaciones
Agentes dirigidos frente al hueso
 Agentes dirigidos frente al hueso IDEAS PRINCIPALES 2. Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, et al. Design and end points of clinical trials for patients with progressive
Agentes dirigidos frente al hueso IDEAS PRINCIPALES 2. Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, et al. Design and end points of clinical trials for patients with progressive
La angiogénesis como factor clave en el tratamiento del cáncer renal tras progresión a un antiangiogénico previo
 La angiogénesis como factor clave en el tratamiento del cáncer renal tras progresión a un antiangiogénico previo Pablo Gajate Borau Oncología Médica Hospital Ramón y Cajal Importancia de la angiogenesis
La angiogénesis como factor clave en el tratamiento del cáncer renal tras progresión a un antiangiogénico previo Pablo Gajate Borau Oncología Médica Hospital Ramón y Cajal Importancia de la angiogenesis
Cáncer de Mama Her2 positivo Situación Actual y Perspectivas de Futuro
 Cáncer de Mama Her2 positivo Situación Actual y Perspectivas de Futuro César A. Rodríguez Servicio de Oncología Médica. Hospital Universitario de Salamanca-IBSAL Introducción HER2 como diana terapéutica
Cáncer de Mama Her2 positivo Situación Actual y Perspectivas de Futuro César A. Rodríguez Servicio de Oncología Médica. Hospital Universitario de Salamanca-IBSAL Introducción HER2 como diana terapéutica
Álvaro Taus Servicio Oncología Hospital del Mar 17 Mayo 2014
 Álvaro Taus Servicio Oncología Hospital del Mar 17 Mayo 2014 Introducción Epidemiología CPCNP Tratamientos dirigidos TERAPIAS ANTI-EGFR Erlotinib Gefitinib Afatinib Caso clínico TERAPIAS ANTI-ALK Crizotinib
Álvaro Taus Servicio Oncología Hospital del Mar 17 Mayo 2014 Introducción Epidemiología CPCNP Tratamientos dirigidos TERAPIAS ANTI-EGFR Erlotinib Gefitinib Afatinib Caso clínico TERAPIAS ANTI-ALK Crizotinib
A PROPÓSITO DE UN CASO: ENFERMEDAD OLIGOMETASTÁSICA
 A PROPÓSITO DE UN CASO: ENFERMEDAD OLIGOMETASTÁSICA Virginia Calvo de Juan Oncología Médica Hospital Universitario Puerta de Hierro Madrid, 26 de Abril de 2016 CÁNCER DE PULMÓN NO CÉLULA PEQUEÑA, ENFERMEDAD
A PROPÓSITO DE UN CASO: ENFERMEDAD OLIGOMETASTÁSICA Virginia Calvo de Juan Oncología Médica Hospital Universitario Puerta de Hierro Madrid, 26 de Abril de 2016 CÁNCER DE PULMÓN NO CÉLULA PEQUEÑA, ENFERMEDAD
Pilar Vázquez Rodríguez Servicio de Medicina Interna B, Complejo Hospitalario Universitario de A Coruña A Coruña, 02/02/2013
 Pilar Vázquez Rodríguez Servicio de Medicina Interna B, Complejo Hospitalario Universitario de A Coruña A Coruña, 02/02/2013 Mayor arsenal terapéutico. Mayor complejidad. Más efectos secundarios. Nuevos
Pilar Vázquez Rodríguez Servicio de Medicina Interna B, Complejo Hospitalario Universitario de A Coruña A Coruña, 02/02/2013 Mayor arsenal terapéutico. Mayor complejidad. Más efectos secundarios. Nuevos
Inhibición irreversible de EGFR: experiencia clínica en primera. EGFR mutado. Edurne Arriola Hospital del Mar Barcelona
 Inhibición irreversible de EGFR: experiencia clínica en primera línea de tratamiento de CPNCP EGFR mutado Edurne Arriola Hospital del Mar Barcelona Inhibición de EGFR Aproximadamente entre un 10 15% de
Inhibición irreversible de EGFR: experiencia clínica en primera línea de tratamiento de CPNCP EGFR mutado Edurne Arriola Hospital del Mar Barcelona Inhibición de EGFR Aproximadamente entre un 10 15% de
F. Dr. Dominguez. Click here if your download doesn"t start automatically
 Carlos J. Finlay. Su centenario (1933). Su descubrimiento (1881). Estado actual de su doctrina (1942). 1º edición en español. Traducción al castellano de Raquel Catalá Click here if your download doesn"t
Carlos J. Finlay. Su centenario (1933). Su descubrimiento (1881). Estado actual de su doctrina (1942). 1º edición en español. Traducción al castellano de Raquel Catalá Click here if your download doesn"t
Reflexive Pronouns. Área Lectura y Escritura
 Reflexive Pronouns Área Lectura y Escritura Resultados de aprendizaje Conocer el uso de los pronombres reflexivos en inglés. Aplicar los pronombres reflexivos en textos escritos. Contenidos 1. Pronombres
Reflexive Pronouns Área Lectura y Escritura Resultados de aprendizaje Conocer el uso de los pronombres reflexivos en inglés. Aplicar los pronombres reflexivos en textos escritos. Contenidos 1. Pronombres
Cáncer de Riñón Avanzado (CRm) A quien y con que tratar en 3ª Línea
 A quien y con que tratar en 3ª Línea") Cáncer de Riñón Avanzado (CRm) A quien y con que tratar en 3ª Línea Hospital Universitario Central de Asturias Servicio de Oncología Médica Emilio Esteban González Cual de estas afirmaciones es más correcta
Cáncer de Riñón Avanzado (CRm) A quien y con que tratar en 3ª Línea Hospital Universitario Central de Asturias Servicio de Oncología Médica Emilio Esteban González Cual de estas afirmaciones es más correcta
Might. Área Lectura y Escritura. In order to understand the use of the modal verb might we will check some examples:
 Might Área Lectura y Escritura Resultados de aprendizaje Conocer el uso del verbo modal might. Aplicar el verbo modal might en ejercicios de escritura. Contenidos 1. Verbo modal might. Debo saber - Verbos
Might Área Lectura y Escritura Resultados de aprendizaje Conocer el uso del verbo modal might. Aplicar el verbo modal might en ejercicios de escritura. Contenidos 1. Verbo modal might. Debo saber - Verbos
What does the polygraph measure?
 What does the polygraph measure? Raymond Nelson July 2015 Qué mide el polígrafo? Raymond Nelson August 2014 In 3000 Words or Less... In 600 words or less In 250 words or less What does the polygraph measure?
What does the polygraph measure? Raymond Nelson July 2015 Qué mide el polígrafo? Raymond Nelson August 2014 In 3000 Words or Less... In 600 words or less In 250 words or less What does the polygraph measure?
Inmunoterapia en cáncer necesitamos una nueva manera de evaluar la eficacia? Elisenda Llabrés Valentí H.U. Insular de Gran Canaria
 Inmunoterapia en cáncer necesitamos una nueva manera de evaluar la eficacia? Elisenda Llabrés Valentí H.U. Insular de Gran Canaria Caso clínico I Mauricio, 58 años AP: -Fumador Febrero 2012 Dx Adenocarcinoma
Inmunoterapia en cáncer necesitamos una nueva manera de evaluar la eficacia? Elisenda Llabrés Valentí H.U. Insular de Gran Canaria Caso clínico I Mauricio, 58 años AP: -Fumador Febrero 2012 Dx Adenocarcinoma
Análisis de la coestimulación vía CD28 en células linfoides de pacientes infectados. con el virus de la Hepatitis C RESUMEN
 Análisis de la coestimulación vía CD28 en células linfoides de pacientes infectados con el virus de la Hepatitis C RESUMEN La infección por el virus de la hepatitis C (VHC) afecta a más de 170 millones
Análisis de la coestimulación vía CD28 en células linfoides de pacientes infectados con el virus de la Hepatitis C RESUMEN La infección por el virus de la hepatitis C (VHC) afecta a más de 170 millones
Evaluate the effect of ProStart PLUS in the flowering response of Cherries plants cv. Bing
 Interpretando El Lenguaje de las Plantas Evaluate the effect of ProStart PLUS in the flowering response of Cherries plants cv. Bing Evaluate the effect of ProStart PLUS in the flowering response of Cherries
Interpretando El Lenguaje de las Plantas Evaluate the effect of ProStart PLUS in the flowering response of Cherries plants cv. Bing Evaluate the effect of ProStart PLUS in the flowering response of Cherries
CONSEJERÍA DE IGUALDAD, SALUD Y POLÍTICAS SOCIALES AGENCIA DE EVALUACIÓN DE TECNOLOGÍAS SANITARIAS DE ANDALUCÍA (AETSA)
") CONSEJERÍA DE IGUALDAD, SALUD Y POLÍTICAS SOCIALES AGENCIA DE EVALUACIÓN DE TECNOLOGÍAS SANITARIAS DE ANDALUCÍA (AETSA) Terapias biológicas en el tratamiento de la espondilitis anquilosante: eficacia y
CONSEJERÍA DE IGUALDAD, SALUD Y POLÍTICAS SOCIALES AGENCIA DE EVALUACIÓN DE TECNOLOGÍAS SANITARIAS DE ANDALUCÍA (AETSA) Terapias biológicas en el tratamiento de la espondilitis anquilosante: eficacia y
Teoría general del proyecto. Vol. I: Dirección de proyectos (Síntesis ingeniería. Ingeniería industrial) (Spanish Edition)
 (Spanish Edition)") Teoría general del proyecto. Vol. I: Dirección de proyectos (Síntesis ingeniería. Ingeniería industrial) (Spanish Edition) Manuel De Cos Castillo Click here if your download doesn"t start automatically
Teoría general del proyecto. Vol. I: Dirección de proyectos (Síntesis ingeniería. Ingeniería industrial) (Spanish Edition) Manuel De Cos Castillo Click here if your download doesn"t start automatically
statutes, etc. Costa Rica. Laws Click here if your download doesn"t start automatically
 COLECCION DE LAS LEYES DECRETOS Y ORDENES EXPEDIDOS POR LOS SUPREMOS PODERES : LEGISLATIVO, CONSERVADOR Y EJECUTIVO DE COSTA RICA, EN LOS AÑOS DE 1833, 1834, 1835 Y 1836. Tomo IV statutes, etc. Costa Rica.
COLECCION DE LAS LEYES DECRETOS Y ORDENES EXPEDIDOS POR LOS SUPREMOS PODERES : LEGISLATIVO, CONSERVADOR Y EJECUTIVO DE COSTA RICA, EN LOS AÑOS DE 1833, 1834, 1835 Y 1836. Tomo IV statutes, etc. Costa Rica.
Thursday, October 5 th.
 7 th. InterAmerican Oncology Conference 'Current Status and Future of Anti-Cancer Targeted Therapies' Estado Actual y Futuro de las Terapias Antineoplásicas October 5-6, 2017 Universidad Católica Argentina
7 th. InterAmerican Oncology Conference 'Current Status and Future of Anti-Cancer Targeted Therapies' Estado Actual y Futuro de las Terapias Antineoplásicas October 5-6, 2017 Universidad Católica Argentina
Introducción al test molecular DecisionDx-MELANOMA
 i Introducción al test molecular DecisionDx-MELANOMA El primer test genético de pronóstico validado para pacientes con melanoma cutáneo en estadios iniciales I y II 1. Datos clínicos 2. Nuestra solución:
i Introducción al test molecular DecisionDx-MELANOMA El primer test genético de pronóstico validado para pacientes con melanoma cutáneo en estadios iniciales I y II 1. Datos clínicos 2. Nuestra solución:
Como cualquier redacción tiene tres párrafos:
 Como cualquier redacción tiene tres párrafos: Introducción (introduction) Desarrollo (body) Conclusión (conclusion) --------------- --------------- --------------- --------------- --------------- ---------------
Como cualquier redacción tiene tres párrafos: Introducción (introduction) Desarrollo (body) Conclusión (conclusion) --------------- --------------- --------------- --------------- --------------- ---------------
Principios generales de actividad de la SEAP
 SEAP-IAP Única sociedad de AP en España, integra SEAP e IAP 1850 miembros, presentes en 350 servicios de AP Cuatro millones de informes clínicos anuales Programa de control calidad propio Acreditación
SEAP-IAP Única sociedad de AP en España, integra SEAP e IAP 1850 miembros, presentes en 350 servicios de AP Cuatro millones de informes clínicos anuales Programa de control calidad propio Acreditación
Aportaciones desde la Anatomía Patológica a la Inmuno-Oncología. Dr. Jose Antúnez López Servicio de Anatomía Patológica
 Aportaciones desde la Anatomía Patológica a la Inmuno-Oncología. Dr. Jose Antúnez López Servicio de Anatomía Patológica Cáncer y Sistema Inmune 1. Alteración de los mecanismos de presentación antigénica.
Aportaciones desde la Anatomía Patológica a la Inmuno-Oncología. Dr. Jose Antúnez López Servicio de Anatomía Patológica Cáncer y Sistema Inmune 1. Alteración de los mecanismos de presentación antigénica.
Aprender español jugando : juegos y actividades para la enseñanza y aprendizaje del español. Click here if your download doesn"t start automatically
 Aprender español jugando : juegos y actividades para la enseñanza y aprendizaje del español Click here if your download doesn"t start automatically Aprender español jugando : juegos y actividades para
Aprender español jugando : juegos y actividades para la enseñanza y aprendizaje del español Click here if your download doesn"t start automatically Aprender español jugando : juegos y actividades para
Nuevos tratamientos para el cáncer de próstata localizado versus prostatectomía. Revisión sistemática
 Nuevos tratamientos para el cáncer de próstata localizado versus prostatectomía. Revisión sistemática Ablación por crioterapia, HIFU y láser New treatments in organ-confined cancer vs. prostatectomy. Systematic
Nuevos tratamientos para el cáncer de próstata localizado versus prostatectomía. Revisión sistemática Ablación por crioterapia, HIFU y láser New treatments in organ-confined cancer vs. prostatectomy. Systematic
INFORME SEOM DE EVALUACIÓN DE FÁRMACOS
 INFORME SEOM DE EVALUACIÓN DE FÁRMACOS para el tratamiento del cáncer de pulmón no microcítico (CPNM) localmente avanzado o metastásico en adultos cuyos tumores expresen PD-L1 y que hayan recibido al menos
INFORME SEOM DE EVALUACIÓN DE FÁRMACOS para el tratamiento del cáncer de pulmón no microcítico (CPNM) localmente avanzado o metastásico en adultos cuyos tumores expresen PD-L1 y que hayan recibido al menos